

Copyrights: Al Hafiz Ibrahim, Muhamad Aizat Mohamed Saat, Mohd Hadizie Din, Nur Sabrina Abdul Ghani, Marne Abdullah, 2024. License: This work is licensed under a Creative Commons Attribution 4.0 International License.
Abstract
Background: Warfarin is a commonly prescribed anticoagulant medication used for thromboprophylaxis in patients at an increased risk of thromboembolic events. However, warfarin administration can lead to hemorrhage due to its narrow therapeutic range. Hemorrhage may occur in unusual anatomical sites and can result in mortality.
Case Presentation: We report the case of an 84-year-old male patient diagnosed with non-valvular atrial fibrillation (AF) and hyperthyroidism, who presented with the sudden onset of lower back pain, bilateral lower limb weakness, and paraesthesia. He was diagnosed with an intramedullary epidural hematoma leading to spinal cord compression as a consequence of overwarfarinization. Following the administration of a new increased dose of oral warfarin, the patient experienced sudden onset back pain accompanied by complete paraplegia. After reversing the overwarfarinization to a therapeutic level, an emergency surgical procedure involving spinal decompression, clot removal, and posterior instrumentation was planned. However, the patient developed an onset of unstable tachyarrhythmia following the administration of anesthesia, leading to the discontinuation of the surgery. Due to substantial risks, the patient declined to undergo the surgical procedure. Despite a consistent neurological condition, he developed a disability and subsequently succumbed to death due to a respiratory infection within four weeks following the initial presentation of symptoms.
Conclusions: This case represents a rare instance of intramedullary epidural hematoma resulting in spinal cord compression due to overwarfarinization, highlighting the need for awareness and urgent management.
Introduction
Warfarin is a conventional oral anticoagulant commonly prescribed for the prevention and treatment of thromboembolic events1. The administration of this medication is frequently recommended for individuals diagnosed with atrial fibrillation (AF), who possess a heightened susceptibility to thromboembolic occurrences. Clinicians face a substantial challenge in achieving a balance between the risks of thrombosis-related events and bleeding complications due to the narrow therapeutic index2. The incidence of bleeding events is notably elevated in the elderly population3. Intraspinal hemorrhage is a severe and potentially life-threatening consequence associated with anticoagulant therapy, although it is rare4. The increased mortality rate observed in individuals with spinal cord injury can be attributed to the occurrence of secondary problems, including infections, pressure sores, and cardiovascular complications5.
Case Presentation
An 84-year-old male patient, diagnosed with non-valvular atrial fibrillation (AF) and hyperthyroidism, presented with sudden onset of lower back pain accompanied by bilateral lower limb weakness and paresthesia. He denied any prior instances of comparable back pain, trauma, or constitutional symptoms. He had a history of hemorrhagic stroke without residual weakness following the event. He was independently ambulant in the community. He complied with warfarin intake and precautions and had no history of bleeding tendencies such as hematuria, hematemesis, or passing melena stools, apart from intracerebral hemorrhage. His international normalized ratio (INR) mostly remained within the range of 2.0-3.0. Nevertheless, one week before this incident, his warfarin dosage was increased from 3.5mg to 4mg due to a subtherapeutic INR.
Clinically, he was alert and conscious with a Glasgow Coma Scale (GCS) of 15/15. His vital signs were within the normal range. No notable abnormalities were exhibited in the cardiovascular, gastrointestinal, and respiratory systems. Peripheral neurological examination indicated a motor function score of 0 out of 5, with diminished sensation observed below the T10 level. His knee and ankle reflexes were absent. Per rectal examination revealed anal tone laxity, absence of deep anal pressure, and lack of anal contraction, with the exception of an intact bulbocavernosus reflex. In contrast, the neurological examination of the bilateral upper limbs were normal.
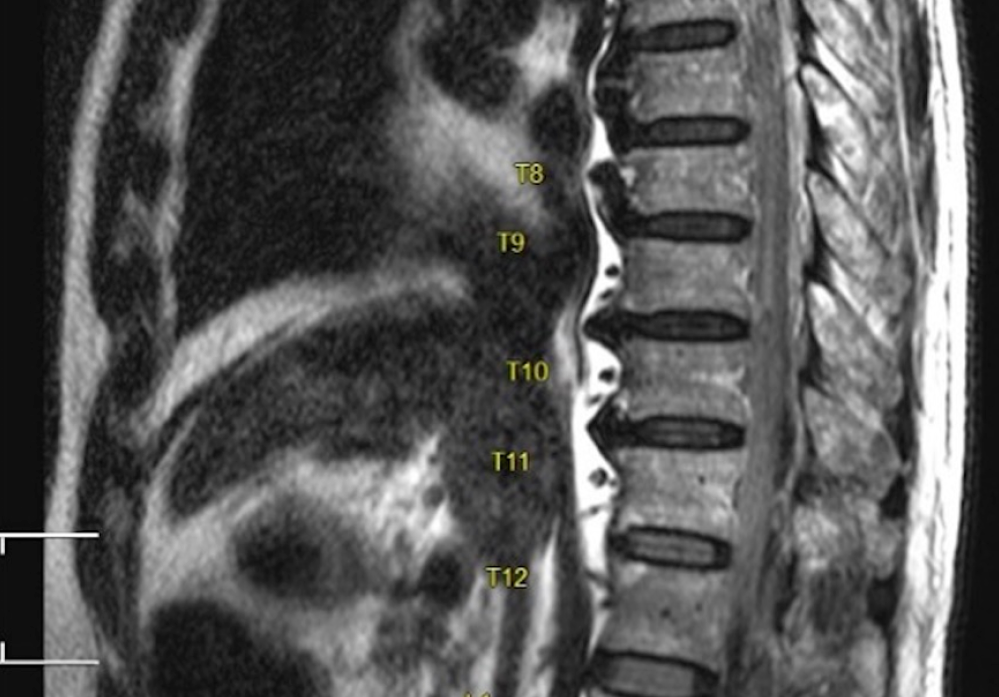
The laboratory investigation indicated an abnormal coagulation profile characterized by an INR of 3.17, a prothrombin time (PT) of 54.9 seconds, and an activated partial thromboplastin time (APTT) of 68.6 seconds. There was no evidence of liver enzyme derangement or electrolyte imbalance. He underwent urgent magnetic resonance imaging (MRI) of the thoracic spine. A distinct linear hypointensity was observed on the T1 image (Figure 1), while hyperintensity was evident on the T2 mage (Figure 2), which was not suppressed on FLAIR and exhibited blooming on the gradient echo sequence (GRE) (Figure 3) within the intramedullary cavity of the T9/T10 region, indicating the presence of a hematoma. It caused stenosis of the spinal canal and anterior compression of the spinal cord at the level of T9, as seen by a hyperintense signal within T2-weighted images (Figure 4).
The administration of warfarin was promptly discontinued, and urgent medical intervention was initiated, involving the transfusion of 4 units of fresh frozen plasma (FFP) and the intravenous administration of 10mg of vitamin K. The surgical decompression procedure was scheduled. Regrettably, the patient experienced the onset of unstable arrhythmias, specifically fast AF, after the induction of anesthesia, resulting in the discontinuation of the surgical procedure.
His neurological level was T-10 according to the ASIA Impairment Scale (AIS), indicating complete loss of sensory and motor function below the T-10 spinal cord segment. Additionally, he exhibited neurogenic bladder and gastrointestinal impairment. Over the course of a ten-day hospitalization, there was no observed improvement in the patient's neurological condition. The implementation of bladder and bowel care was facilitated by a multidisciplinary team, including the rehabilitation team. He opted to return to his residence for further care. The patient was discharged in a bed-bound state, with re-admission scheduled the following week for rehabilitation training. Nevertheless, the patient’s health deteriorated at home, ultimately resulting in his demise due to a respiratory infection approximately four weeks after the initial manifestation of back pain.




Discussions
Atrial fibrillation is a common cardiac arrhythmia observed in the general population and is associated with increased cardiac-related morbidity and mortality6. Warfarin, an oral anticoagulant that acts as a vitamin K antagonist, is commonly prescribed for the prevention of thromboembolic complications associated with atrial fibrillation1. However, due to its narrow therapeutic index, there is a risk of unintended overwarfarinization, which can lead to bleeding complications. These complications can range from catastrophic outcomes to substantial morbidity7, 8. Warfarin therapy has been demonstrated to be safe and effective in the management of thromboembolic-related illnesses, as long as it is maintained within the therapeutic range9.
Our case involved an increased risk for bleeding due to extreme age and previous intracranial bleeding. Close INR monitoring was imperative to balance the therapeutic effect and the risk of bleeding. An INR level above 3 frequently leads to hemorrhage, but insufficient anticoagulation with an INR level below 2 increases the likelihood of thrombotic events10. Surprisingly, slight overwarfarinization of 3.17 had caused a clinically significant amount of an intraspinal hematoma in our case. Considering the identified risk factors for bleeding in this case, an alternative choice for an anticoagulant is a direct oral anticoagulant (DOAC). Nonetheless, it is worth noting that the associated expenses are comparatively elevated11.
Spontaneous intraspinal hemorrhage is a relatively infrequent condition that can be categorized based on its anatomical location, including epidural, subdural, subarachnoid, or intramedullary. Among the many types, the intramedullary type, known as hematomyelia, was shown to be a rather unusual occurrence4. It is considered spontaneous if not related to trauma, surgery, arteriovenous malformation, malignancy, or lumbar puncture12. Nevertheless, the use of anticoagulant therapy has been identified as a potential causative factor in the development of intraspinal hemorrhage. In the context of warfarin therapy, the occurrence of intraspinal hemorrhage might lead to atypical clinical manifestations as a result of the gradual nature of the bleeding process8. Conversely, a clinician should be alerted to the possibility of intraspinal hemorrhage when a patient undergoing warfarin therapy complains of sudden onset of back pain or neurological impairment. Magnetic resonance imaging (MRI) is often regarded as the optimum modality for radio-imaging due to its ability to effectively visualize the spinal cord and detect abnormalities13. There is no consensus regarding the treatment of intraspinal hemorrhage secondary to overwarfarinization. The evidence highlights that early intervention by the administration of fresh frozen plasma or vitamin K can effectively mitigate the progression of hematoma and enhance neurological function8. Non-surgical intervention may be considered a viable option in cases where there is partial neurological impairment or if there is observed improvement in neurological deficits within a 24-hour period after the reversal of coagulopathy. In certain instances, surgical intervention may be warranted as a means of mitigating additional neurological decline14. According to the literature, there is evidence to suggest that the neurological outcomes of patients may be enhanced when surgical intervention is conducted within a timeframe of 12 hours following the onset of symptoms15.
Conclusions
The condition known as intramedullary hematomyelia is a neurological emergency that necessitates expeditious diagnosis and treatment. This case highlights the critical importance of timely intervention and comprehensive care. Prompt reversal of coagulopathy is necessary prior to the initiation of surgical intervention. The use of a multidisciplinary strategy and the effective management of rehabilitation play a crucial role in enhancing clinical outcomes and mitigating the occurrence of secondary complications leading to mortality.
Abbreviations
AF - Atrial Fibrillation, AIS - ASIA Impairment Scale, APTT - Activated Partial Thromboplastin Time, DOAC - Direct Oral Anticoagulant, FFP - Fresh Frozen Plasma, FLAIR - Fluid-Attenuated Inversion Recovery, GCS - Glasgow Coma Scale, GRE - Gradient Echo Sequence, INR - International Normalized Ratio, MRI - Magnetic Resonance Imaging, PT - Prothrombin Time, T - Thoracic
Acknowledgments
Acknowledgement are due to Hospital Universiti Sains Malaysia for allowing this case to be presented.
Author’s contributions
A.H.I and M.A.M.S contributed in the conception and wrote of the case report. M.H.D and N.S.A.G are involved in management of the patients and acquisition of clinical data. M.A contributed to laboratory data interpretation and discussion. All authors reviewed and approved the final manuscript.
Funding
None.
Availability of data and materials
Data and materials used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics approval and consent to participate
Not necessary for this manuscript.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Competing interests
The authors declare that they have no competing interests.
References
-
Johnson
J.A.,
Caudle
K.E.,
Gong
L.,
Whirl-Carrillo
M.,
Stein
C.M.,
Scott
S.A.,
Clinical Pharmacogenetics Implementation Consortium (CPIC) guideline for pharmacogenetics-guided warfarin dosing: 2017 update. Clinical Pharmacology and Therapeutics.
2017;
102
(3)
:
397-404
.
View Article PubMed Google Scholar -
Hylek
E.M.,
Skates
S.J.,
Sheehan
M.A.,
Singer
D.E.,
An analysis of the lowest effective intensity of prophylactic anticoagulation for patients with nonrheumatic atrial fibrillation. The New England Journal of Medicine.
1996;
335
(8)
:
540-6
.
View Article PubMed Google Scholar -
Shendre
A.,
Parmar
G.M.,
Dillon
C.,
Beasley
T.M.,
Limdi
N.A.,
Influence of Age on Warfarin Dose, Anticoagulation Control, and Risk of Hemorrhage. Pharmacotherapy.
2018;
38
(6)
:
588-96
.
View Article PubMed Google Scholar -
Pullarkat
V.A.,
Kalapura
T.,
Pincus
M.,
Baskharoun
R.,
Intraspinal hemorrhage complicating oral anticoagulant therapy: an unusual case of cervical hematomyelia and a review of the literature. Archives of Internal Medicine.
2000;
160
(2)
:
237-40
.
View Article PubMed Google Scholar -
Krassioukov
A.V.,
Furlan
J.C.,
Fehlings
M.G.,
Medical co-morbidities, secondary complications, and mortality in elderly with acute spinal cord injury. Journal of Neurotrauma.
2003;
20
(4)
:
391-9
.
View Article PubMed Google Scholar -
Pistoia
F.,
Sacco
S.,
Tiseo
C.,
Degan
D.,
Ornello
R.,
Carolei
A.,
The Epidemiology of Atrial Fibrillation and Stroke.. Cardiology clinics.
2016;
34
(2)
:
255-68
.
View Article Google Scholar -
Hosseini
M.,
Hosseinzadeh
A.,
Raufian
K.,
Hedjazi
A.,
Nontraumatic retroperitoneal hematoma after warfarin administration: fatal case report and review of the literature. The American Journal of Forensic Medicine and Pathology.
2015;
36
(4)
:
245-8
.
View Article PubMed Google Scholar -
Inamasu
J.,
Ito
K.,
Hattori
N.,
Hirose
Y.,
Warfarin-associated intraspinal hematoma. The Keio Journal of Medicine.
2016;
65
(4)
:
74-7
.
View Article PubMed Google Scholar -
Sjögren
V.,
Grzymala-Lubanski
B.,
Renlund
H.,
Friberg
L.,
Lip
G.Y.,
Svensson
P.J.,
Safety and efficacy of well managed warfarin. A report from the Swedish quality register Auricula. Thrombosis and Haemostasis.
2015;
113
(6)
:
1370-7
.
View Article PubMed Google Scholar -
Shi
C.,
Yan
W.,
Wang
G.,
Wang
F.,
Li
Q.,
Lin
N.,
Pharmacogenetics-based versus conventional dosing of warfarin: A meta-analysis of randomized controlled trials. PLoS One.
2015;
10
(12)
:
e0144511
.
View Article PubMed Google Scholar -
Tan
S.K.,
Looi
W.L.,
Yeo
H.Y.,
Estimation of direct medical costs of warfarin, dabigatran and rivaroxaban treatments in non-valvular atrial fibrillation patients in a tertiary public hospital, Malaysia. Journal of Pharmacy Practice and Research.
2020;
50
(5)
:
406-12
.
View Article Google Scholar -
Heppner
P.A.,
Monteith
S.J.,
Law
A.J.,
Spontaneous spinal hematomas and low-molecular-weight heparin. Report of four cases and review of the literature. Journal of Neurosurgery. Spine.
2004;
1
(2)
:
232-6
.
View Article PubMed Google Scholar -
Leep Hunderfund
A.N.,
Wijdicks
E.F.,
Intramedullary spinal cord hemorrhage (hematomyelia). Reviews in Neurological Diseases.
2009;
6
(2)
:
54-61
.
PubMed Google Scholar -
Famularo
G.,
Sajeva
M.R.,
Gasbarrone
L.,
Warfarin-associated hematomyelia. Internal Medicine (Tokyo, Japan).
2014;
53
(6)
:
623-6
.
View Article PubMed Google Scholar -
Mukerji
N.,
Todd
N.,
Spinal epidural haematoma; factors influencing outcome. British Journal of Neurosurgery.
2013;
27
(6)
:
712-7
.
View Article PubMed Google Scholar
Comments
Article Details
Volume & Issue : Vol 11 No 9 (2024)
Page No.: 6786-6791
Published on: 2024-09-30
Citations
Copyrights & License
This work is licensed under a Creative Commons Attribution 4.0 International License.
Search Panel
Pubmed
Google Scholar
Pubmed
Google Scholar
Pubmed
Google Scholar
Pubmed
Google Scholar
Pubmed
Search for this article in:
Google Scholar
Researchgate
- HTML viewed - 1594 times
- PDF downloaded - 601 times
- XML downloaded - 70 times
