

Copyrights: Manna Sulagna, Raju Kalyani, Mohiyuddin Azeem, 2018. License: This work is licensed under a Creative Commons Attribution 4.0 International License.
Abstract
Fibrosarcoma of bone occur in any location but mainly affects long bone. Its occurrence in craniofacial region is about 15%, mandible being the most common site. Fibrosarcoma of hed and neck area represents 5% of all malignant intraosseous tumours. It is commonly seen between 3rdto 6thdecades of life. Here we present a case in 65 years old female with past history of radiotherapy for carcinoma of buccal mucosa and now presents with fibrosarcoma of the left jaw which was diagnosed by FNAC and confirmed by biopsy.
Background
Fibrosarcoma is a malignant spindle cell neoplasm. Soft tissue sarcomas are rare in the oral and maxillofacial region and account for less than 1% of the cancers. Fibrosarcoma is the most common soft tissue sarcoma. It constitutes about 5% of head and neck malignant osseous tumours. Its occurrence in craniofacial region is about 15%, mandible being the most common site. The cause for primary fibrosarcoma is not exactly known. However, there are a few proved risk factors for fibrosarcoma presenting as a secondary malignant tumour [1][2].
Case History
65 years female presented with the history of swelling in left jaw since one month ( Figure 1 ). Swelling of the jaw was insidious in onset, gradually progressive and associated with dull aching pain, non-radiating without any aggravating and relieving factors. Patient had difficulty in articulation. Patient gives a history of tooth extraction once, six months back and second time two months back. Past history revealed that the patient had undergone right hemimandibulectomy surgery eight years back for carcinoma of buccal mucosa and radiotherapy was given to the patient post-operatively. Family history was not significant. On examination, the swelling was present on left side in mandibular region measuring 6x5x5 cms. Overlying skin was stretched. Intraorally the tumour extended into the oral cavity and was firm in consistency, nodular with ulceration of buccal mucosa. The tumour was fixed to the bone. There was no evidence of any palpable cervical lymph nodes.

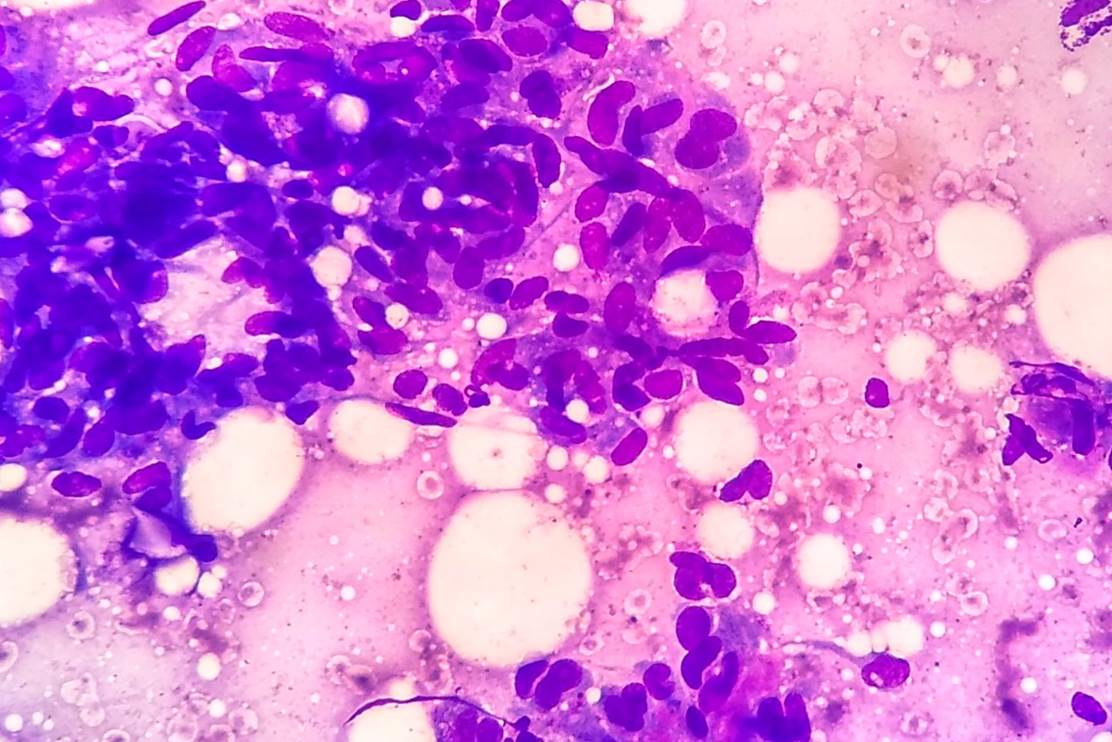
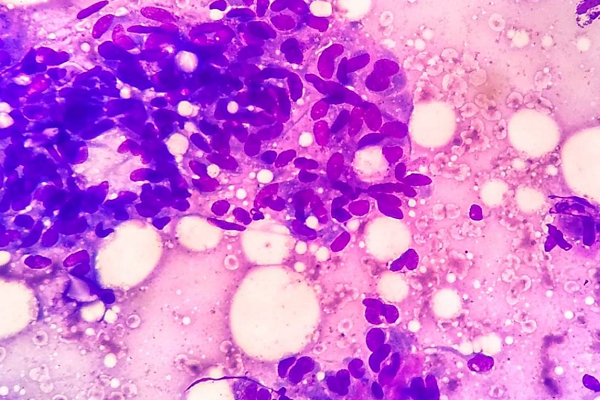
Patient was subjected to FNAC of jaw tumour. Smears studied from the aspirate showed moderately cellular smear consisting of pleomorphic spindle cells arranged in groups, clusters and in singles. The cells had increased nucleus to cytoplasmic ratio, elongated nuclei with moderate amount of cytoplasm ( Figure 2 ). A few giant cells were also seen. A Cytological diagnosis of spindle cell tumor was given.
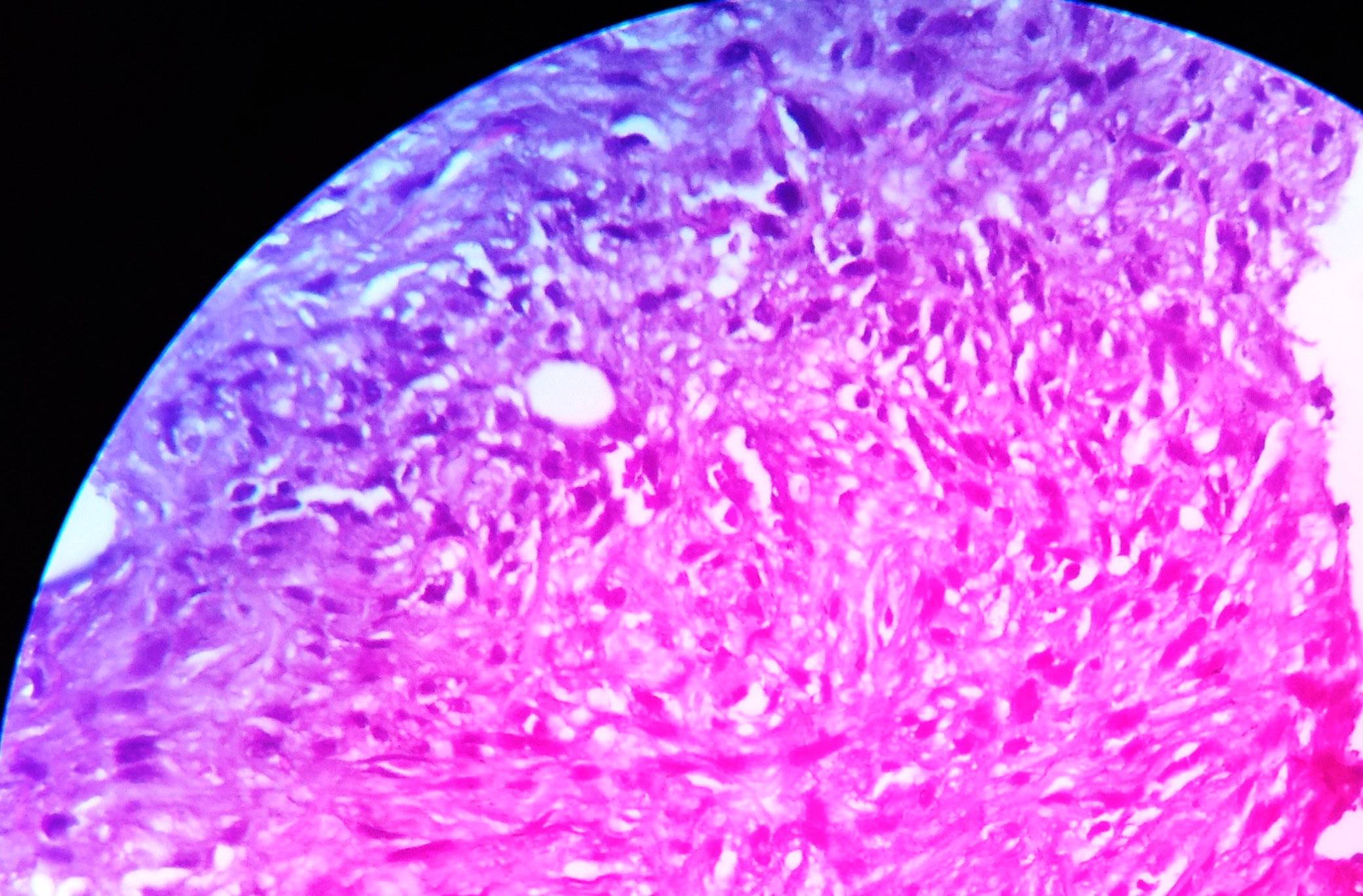
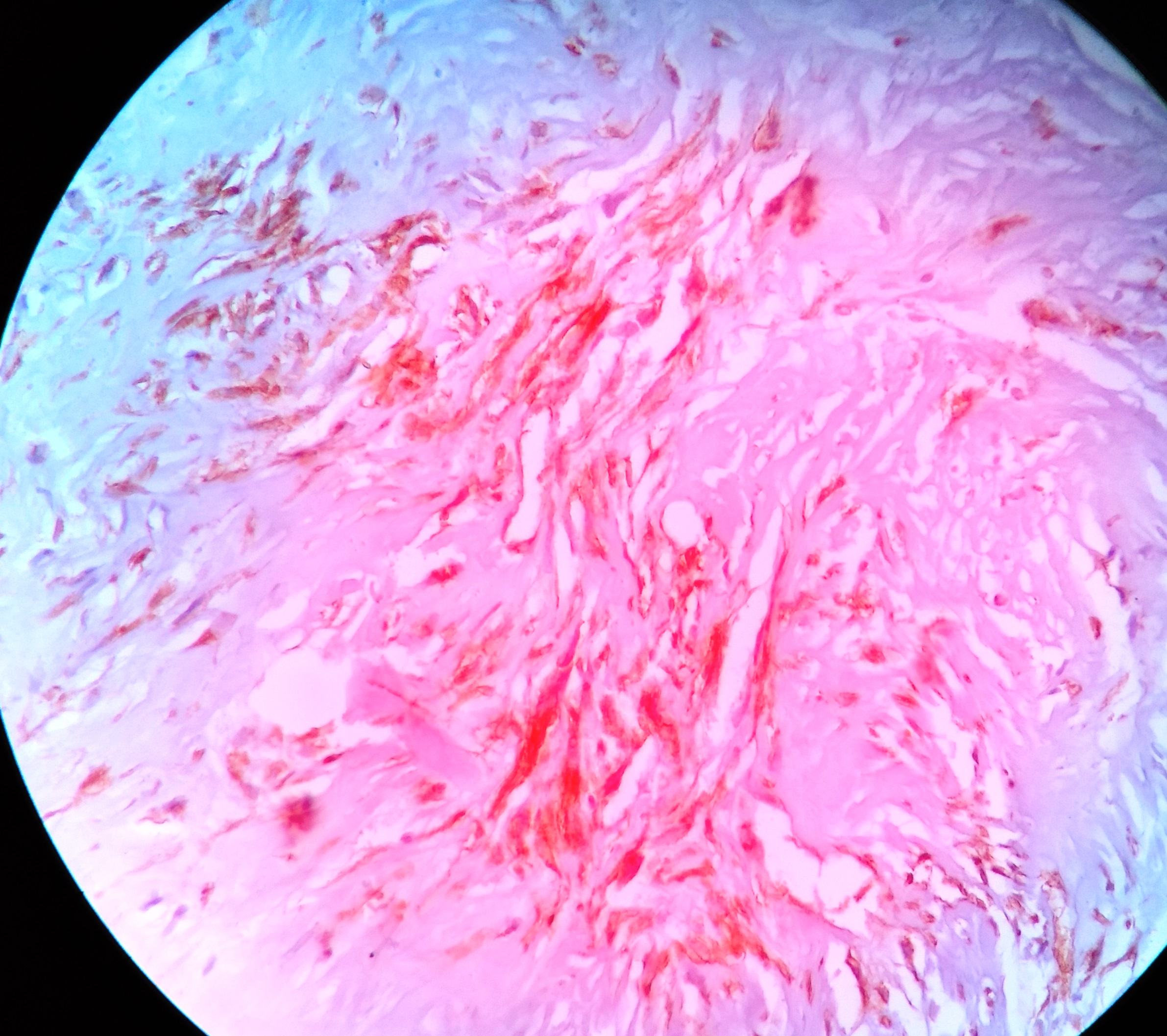
Patient was subjected to trucut biopsy. Section studied from trucut biopsy showed highly pleomorphic spindle cells with hyperchromatic nucleus and irregular nuclear border. Occasional monocytoid tumor giant cell were seen. Cells were arranged in intersecting fascicles ( Figure 3 and Figure 4 ). Stroma showed of dense fibrocollagenous tissue. Other fragments showed focal areas of necrosis. Mitotic figures were few in number. A Histopathological diagnosis of Fibrosarcoma of Mandible-Low Grade was offered.Tissue block was subjected for immunohistochemistry which showed strong positivity to vimentin, ( Figure 5 ) focally positive for cytokeratin and S-100 and negative for CD-34. A final diagnosis of fibrosarcoma of mandible was offered.

Patient was referred to cancer center for treatment and was lost for follow up.
Discussion
Fibrosarcoma is the malignant tumour of fibroblastic origin. It is rare in oral and oropharyngeal region. It occurs in any location but mainly affects long bone. Its occurrence in craniofacial region is about 15%, mandible being the most common site. Although fibrosarcoma has been reported in all groups, it is most commonly seen in the 3rd to 6th decades of life. It is seen equally in males and females [1][3]. In our case, the patient was 65 years female and presented with the tumour in left mandible.
The clinical presentation depends on location, size and spread of tumour. In jaw the tumour presents with pain or without pain, swelling, paresthesia, ulceration of overlying mucosa and difficulty in articulation. Paresthesia is late manifestation of the tumour indicating nerve involvement [1][4]. In the present case the patient presented with the swelling, pain and difficulty in articulation.
The exact cause for this tumour is not known. Genetic alteration is thought to be one of the mechanisms. Fibrosarcoma presenting as a secondary primary tumor has been reported. The causes are fibrous dysplasia, Paget’s disease, bone infarct or cyst, osteomyelitis, malignant transformation of giant cell tumour of bone and post-radiation [1][5]. The latent period between radiotherapy and the diagnosis of the tumour ranges from 3-38 years [4]. In our case, it is post-irradiation done for primary carcinoma of buccal mucosa and the latent period was 8 years. Intra-osseous fibrosarcomas may develop endosteally or possibly periosteally, in the latter cases the bones are affected by spread from adjacent soft tissues. In jaw it may erode into the roots of the involved teeth [1][3][5]. In our case the tumor was arising from the left mandible and was extending into the soft tissue. Patient had history of teeth extraction.
Fibrosarcoma are graded into low to high grade of malignancy depending on the number of mitosis, tumour differentiation and presence of tumour necrosis [1][4]. Our case was a low grade fibrosarcoma.
The differential diagnosis histomorphologically are other spindle cell tumours. However IHC markers help in precise diagnosis [1]. IHC markers like Vimentin, S-100, Cytokeratin cocktail, HMB-45, Desmin, Smooth Muscle Actin shows positivity for fibrosarcoma [4][5]. In the present 5 case tumour showed strong positivity to vimentin, focally positive for cytokeratin and S-100 and negative for CD-34.
Treatment of choice is radical surgery. Radiotherapy and chemotherapy are used for high grade tumours or inoperable cases. The overall ten year survival rate varies from 21.8% to 83%. Clinical stage, histological grade and local recurrences are important prognostic factors. The prognosis depends on the tumour grade and the success of complete excision. The need for adjuvant radiotherapy and/or chemotherapy is still unclear. High grade tumours present with subclinical or microscopic metastases at the time of diagnosis and the prognosis is fatal [1][4][5]. In the present case the patient was referred to cancer center for treatment and lost for follow up.
Conclusion
Fibrosarcoma is a rare malignancy of head and neck region. Ours is a unique case where the tumour was presented as second primary malignancy following radiotherapy for carcinoma of buccal mucosa.
Open Access
This article is distributed under the terms of the Creative Commons Attribution License (CC-BY 4.0) which permits any use, distribution, and reproduction in any medium, provided the original author(s) and the source are credited.
List of abbreviations
CD: Cluster designation or cluster of differentiation ; FNAC: Fine needle aspiration cytology;
H&E: Hematoxylin and Eosin; HMB: Human melanoma black ; IHC: Immunohistochemistry
Ethics approval and consent to participate
Institutional ethical clearance for publication
Availability of data and materials
None
Competing interests
The authors have declared that no conflict of interest exists.
Funding
None
Authors’ contributions
Manna Sulagna: Literature search, Clinical studies, Data acquisition, Data analysis, Manuscript preparation; Raju Kalyani: Concepts, Design, Definition of intellectual content, Literature search, Clinical studies, Data acquisition, Data analysis, Manuscript preparation, Manuscript editing, Manuscript review, Guarantor; Mohiyuddin Azeem: Clinical studies, Data analysis, Manuscript editing, Manuscript review.
References
-
AS
Sachdev,
M
Asdullah,
A
Sachdev,
M
Naeem.
FIBROSARCOMA OF THE MANDIBLE. University Journal of Dental Sciences.
2015;
1(2)
:
74-76
.
-
M
Gosau,
FG
Draenert,
WA
Winter,
J
Mueller-Hoecker,
O
Driemel.
Fibrosarcoma of the childhood mandible. Head & face medicine.
2008;
4
:
21
.
View Article PubMed PMC Google Scholar -
MB
Yuwanati,
JV
Tupkari.
Fibrosarcoma of mandible: a case report. Case reports in dentistry 2011.
2011
.
View Article Google Scholar -
KDS
Nanda,
A
Mehta,
J
Nanda.
Fibrosarcoma of the mandible: a diagnostic dilemma. Journal of clinical and diagnostic research: JCDR.
2013;
7
:
1804
.
View Article Google Scholar -
AB
Soares,
LHS
Lins,
AP
Mazedo,
JSP
Neto,
PA
Vargas.
Fibrosarcoma originating in the mandible. Medicina Oral, Patología Oral y Cirugía Bucal (Internet).
2006;
11
:
243-246
.
Comments
Downloads
Article Details
Volume & Issue : Vol 5 No 5 (2018)
Page No.: 2326-2331
Published on: 2018-05-22
Citations
Copyrights & License
This work is licensed under a Creative Commons Attribution 4.0 International License.
Search Panel
Pubmed
Google Scholar
Pubmed
Google Scholar
Pubmed
Search for this article in:
Google Scholar
Researchgate
- HTML viewed - 11082 times
- Download PDF downloaded - 2088 times
- View Article downloaded - 0 times

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}