

Copyrights: Mahdi Mohammadian, Mahin Ghafari, Bahman Khosravi, Hamid Salehiniya, Mohammad Aryaie, Fatemeh Allah Bakeshei, Abdollah Mohammadian-Hafshejani, 2017. License: This work is licensed under a Creative Commons Attribution 4.0 International License.
Abstract
Background: Ovarian cancer (OC) has high incidence and mortality rates among the reproductive system cancers. This study investigated the relationship between the age-standardized incidence rate (ASIR) and age-standardized mortality rate (ASMR) of OC and Human Development Index (HDI) in European countries in 2012.
Methods: This ecological study assessed the correlation between the ASIR and ASMR of OC and HDI and its components including life expectancy at birth, average years of schooling, and gross national income (GNI) per capita. Bivariate correlation analysis was used for assessing the correlation between the ASIR and ASMR of OC and HDI and its components. All reported P values were two-sided. Statistical analyses were performed using SPSS (Version 15.0, SPSS Inc.).
Results: The maximum ASIR of OC was observed in Latvia, Bulgaria, and Poland. The highest ASMR of OC was observed in Latvia, Lithuania, and Poland. The incidence and mortality rates of OC are expected to increase between 2012 and 2035. This increase will be more pronounced in women ≥ 65 years. HDI had a weak negative correlation with the ASIR of OC (r=- 0.213; P=0.186) and a weak positive correlation with the ASMR of OC (r=0.072; P=0.659).
Conclusion: According to the results of this study, health policy makers must make appropriate decisions to deal with the increasing morbidity and mortality of OC, especially in women over 65 years of age, in regions with lower access to prevention and treatment services.
Introduction
Ovarian cancer (OC) is the seventh leading cancer diagnosis and the fifth leading cause of cancer-related mortalities Coburn et al., 2017. OC has high incidence and mortality rates among the reproductive system cancers Ferlay et al., 2010. Based on the global estimates, about 225,000 new cases of OC are diagnosed every year and 140,000 women annually die from this disease worldwide Ferlay et al., 2010. In 2014, the lifetime risk of OC among women in the United States was ranging from 4% to 9%, 73% of women had no family history of ovarian cancer Pearce et al., 2015.
The incidence and mortality rates of OC vary in different areas of the world Coburn et al., 2017. Although the incidence and mortality rates of OC are globally high, the cause and etiology of the disease are not completely understood Razi et al., 2015. However, several factors associated with OC have been identified and classified into three categories of protective factors, e.g. parity and contraceptive use, risk factors, e.g. no history of a full-term pregnancy, a positive family history of OC, and age, and other factors, e.g. such as lactation, age at menopause, and age at menarche, whose relations with OC are not clearly determined Poorolajal et al., 2014. One of the significant factors related with OC is the Human Development Index (HDI) which reflects the socioeconomic position of individuals living in different countries Mahdavifar et al., 2016Mohammadian et al., 2015Shuja et al., 2017.
Socioeconomic factors affect cancer incidence and mortality through complex and changeable mechanisms. In a study in Asian countries in 2012, Razi et al. found a positive correlation between age-standardized incidence rate (ASIR) of OC and HDI and its components including life expectancy at birth, average years of schooling, and gross national income (GNI) per capita. However, no significant correlation was observed between age-standardized mortality rate (ASMR) of OC and HDI and its components Razi et al., 2016. While several other studies have evaluated the relationship between HDI and various cancers, especially in Asian countries Ghoncheh et al., 2015Hassanipour-Azgomi et al., 2016Mohammadian et al., 2015Pakzad et al., 2015a, bPakzad et al., 2016Rafiemanesh et al., 2015, the relationships between the incidence and mortality of OC and HDI have not been assessed in European countries. Therefore, this study aimed to investigate the relationship between the ASIR and ASMR of OC with HDI and its components, i.e. life expectancy at birth, the average years of schooling, and the country’s GNI per capita in 2012. We used HDI as an indicator of socioeconomic development Bray et al., 2012.
Materials - Methods
This ecological study examined the relationship between ASIR and ASMR of OC and HDI and its components including life expectancy at birth, average years of schooling, and GNI per capita. The 2012 ASIR and ASMR data for each European country were collected from the GLOBOCAN project (available at http://globocan.iarc.fr/Default.aspx) Ferlay et al., 2015. Data about the HDI were extracted from the Human Development Report 2013 (Malik, 2013). The details of the methods to estimate the ASIR and ASMR in GLOBOCAN project have been provided in previous reports Ferlay et al., 2010Ferlay et al., 2015Foulkes and Cooney, 2010Pakzad et al., 2015bPakzad et al., 2016.
Statistical analysis: Pearson’s correlation analysis was used to assess the correlations between the ASIR and ASMR of OC and HDI and its components. All reported ASIR and ASMR were per 100,000. Statistical significance was considered at P ≤ 0.05. All P values reported in this study are two-sided. All statistical analyses were performed using SPSS 15.0 (SPSS Inc., Chicago, IL, USA).
Results
A total of 65584 cases of OC were recorded in European countries in 2012. Five countries, including the Russian Federation (13,373 cases), the United Kingdom (6,692 cases), Germany (6,673 cases), Italy (5,911 cases) and France (metropolitan; 4,592 cases), had the highest numbers of OC. Overall, 37,241 cases (56.78%) of OC were reported in these five countries.
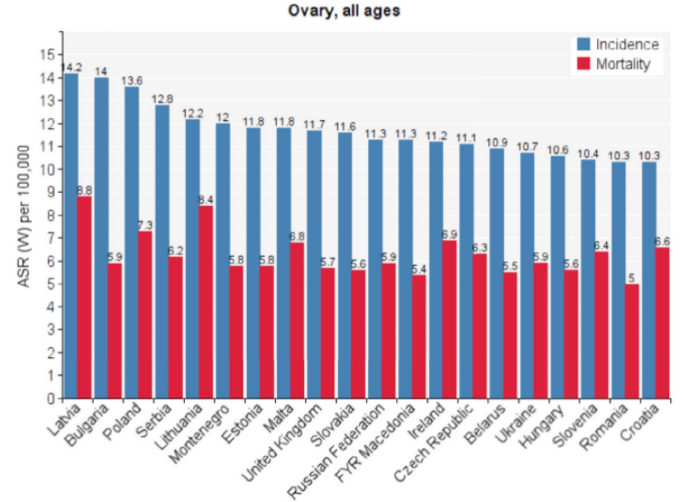
The highest ASIRs of OC were seen in Latvia (14.2 per 100,000), Bulgaria (14 per 100,000), Poland (13.6 per 100,000), Serbia (12.8 per 100,000), and Lithuania (12.2 per 100,000). The lowest ASIRs of the OC belonged to Albania (3.2 per 100,000), Ireland (6 per 100,000), Portugal (6.2 per 100,000), the Netherlands (6.5 per 100,000), and Cyprus (7 per 100,000). The number, crude incidence rate, and ASIR of the OC based on sex are presented in Table 1 . The countries with the highest and lowest ASIR in both sexes are shown in Table 1 , Figure 1 , and Figure 3 .
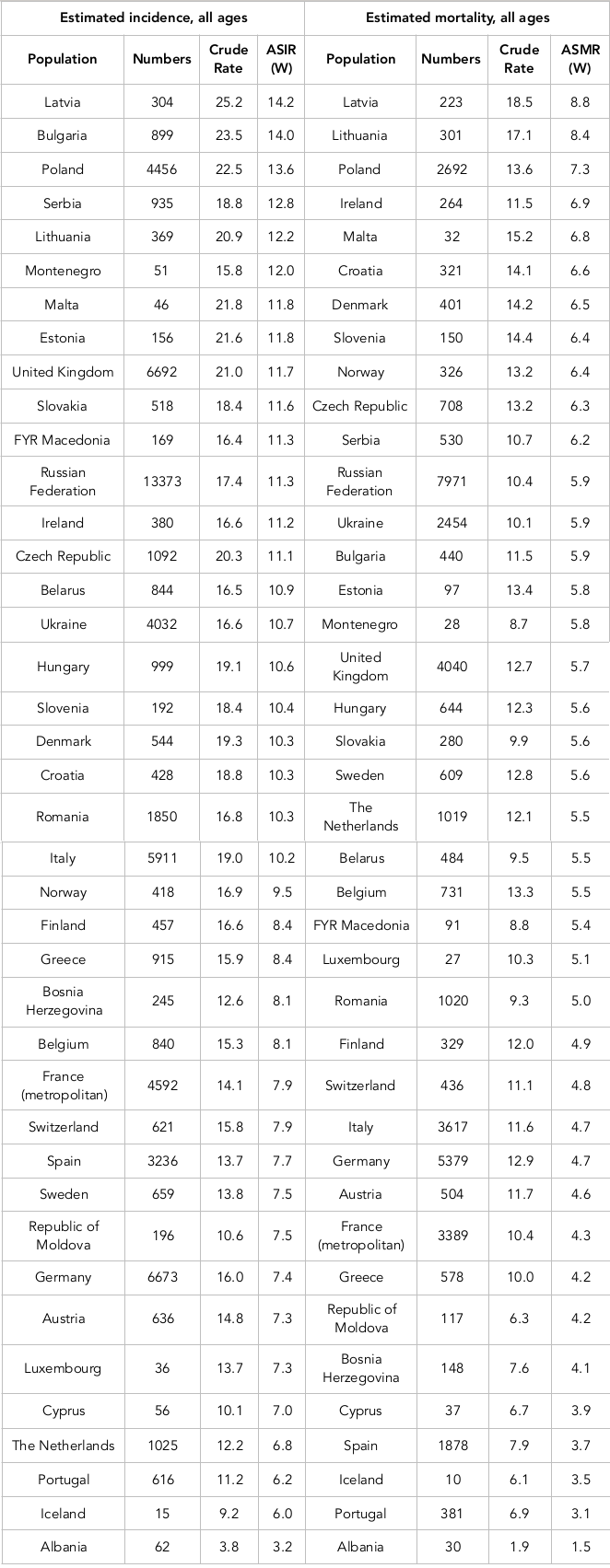

A total of 42,749 deaths due to OC were recorded in 2012. The Russian Federation (7,971 cases), Germany (5,379 cases), the United Kingdom (4,040 cases), Italy (3,617 cases) and France (metropolitan; 3,389 cases) were the five countries with the highest numbers of deaths. Overall, 57.06% of deaths due to OC occurred in these five countries.
Latvia (8.8 per 100,000), Lithuania (8.4 per 100,000), Poland (7.3 per 100,000), Ireland (6.9 per 100,000), and Malta (6.8 per 100,000) had the highest ASMRs of OC. Albania (1.5 per 100,000), Portugal (3.1 per 100,000), Iceland (3.5 per 100,000), Spain (3.7 per 100,000), and Cyprus (3.9 per 100,000) had the lowest ASMRs of OC ( Table 2 , Figure 2 and Figure 3 ).
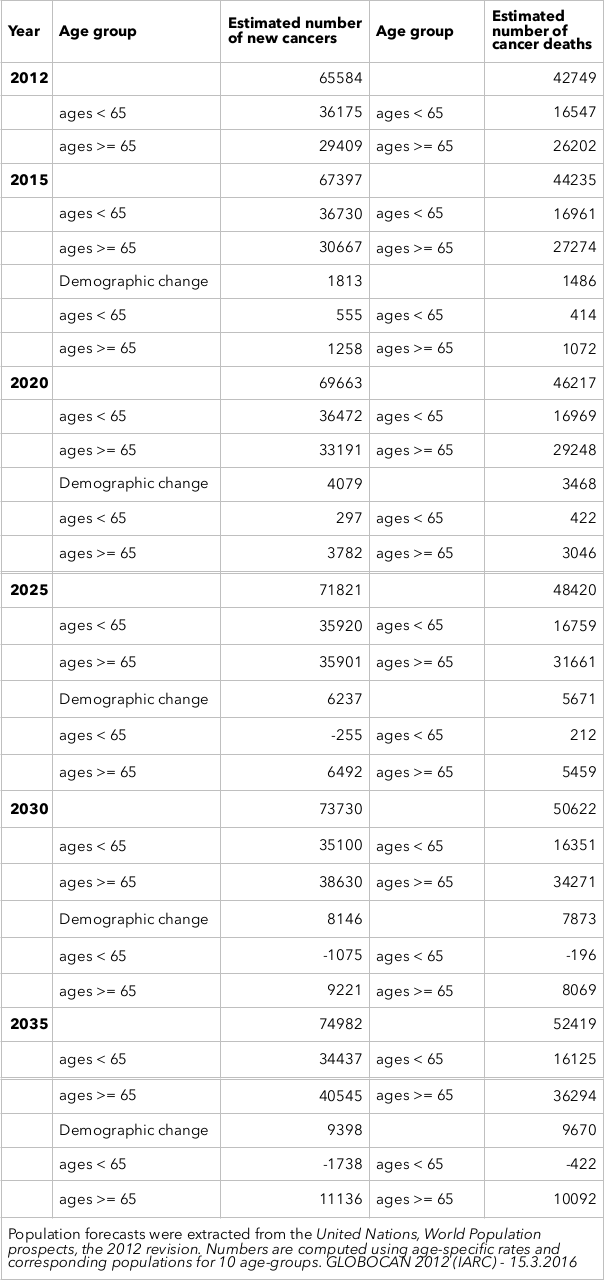

Of the 65,584 new cases of OC reported in 2012, 36,175 cases (55.15%) were in women below 65 years old and 29,409 cases (44.85%) were in those 65 years old or older. The numbers of new cases of OC in 2015, 2020, 2025, 2030, and 2035 are predicted to be 67,397, 69,663, 71,821, 73,730 and 74,982, respectively. These numbers are respectively 1,813 (2.76%), 4,079 (6.21%), 6,237 (9.50%), 8,146 (12.42%), and 9,398 (14.32%) higher than the new cases in 2012. While the number of new cases of OC is expected to increase in women ≥ 65 years old during 2012-2035, it is predicted to decrease in the age group below 65 years.
Of the 42,749 deaths due to OC in 2012, 16,547 (38.70%) and 26,202 deaths (61.30%) belonged to the age groups < 65 years and ≥ 65 years, respectively. The numbers of deaths due to OC are expected to reach 44,235, 46,217, 48,420, 50,622, and 52419 in 2015, 2020, 2025, 2030, and 2035, respectively. These numbers are 1,486 (3.47%), 3,468 (8.11%), 5,671 (13.26%), 7,873 (18.41%), and 9,670 (22.62%) higher than the rate reported in 2012. Apparently, the number of deaths due to OC is expected to increase between 2012 and 2035 and this increase is predicted to be more pronounced in women ≥ 65 years old.
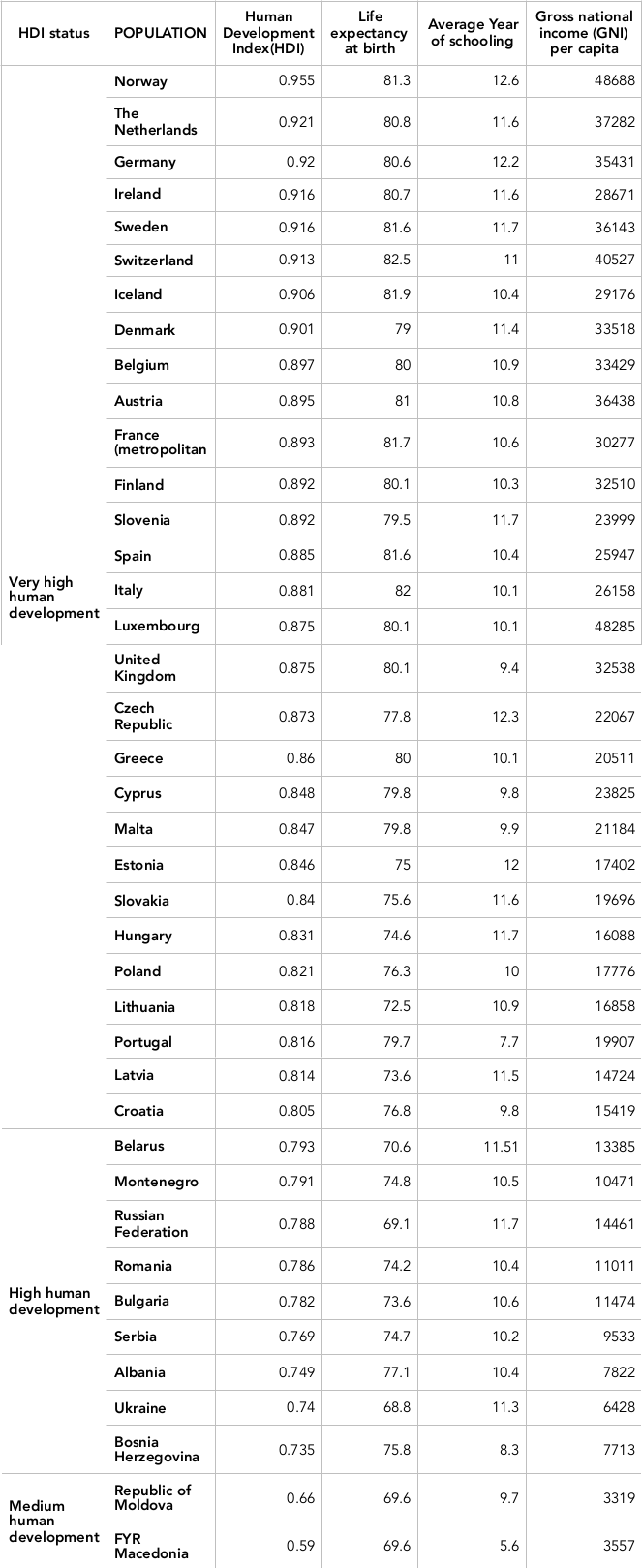
Table 3 shows the HDI and its components in 2012. Accordingly, the European countries were classified to have very high HDI (n = 29), high HDI (n = 9), and moderate HDI (n = 2).
ASIR and HDI
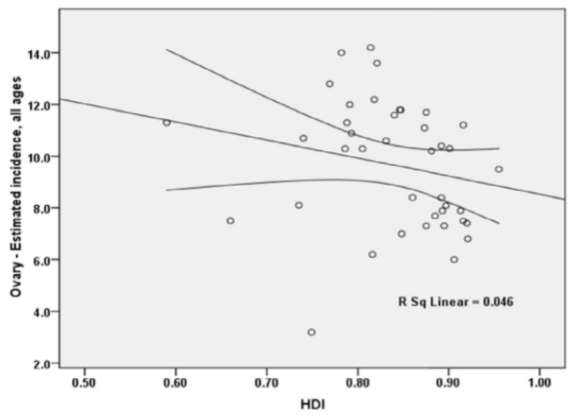
A weak negative correlation was seen between the HDI and the ASIR of OC (r = -0.213; P = 0.186). There was a strong negative correlation between life expectancy at birth and the ASIR of OC (r = -0.480; P = 0.002). The mean years of schooling and the ASIR of OC had a weak positive correlation (r = 0.115; P = 0.481). Moreover, the GNI per capita and the ASIR of OC had a strong negative correlation (r = -0.348; P = 0.028) ( Figure 4 ).
ASMR and HDI
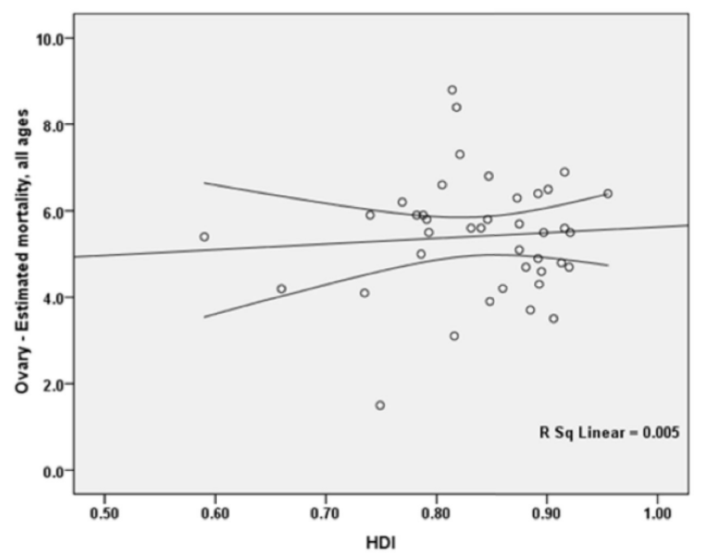
There was a weak positive correlation between the HDI and the ASMR of OC (r = 0.072; P = 0.659). Meanwhile, life expectancy at birth and the ASMR of OC were negatively correlated (r = -0.275; P = 0.086). A strong positive correlation was seen between the mean years of schooling and the ASMR of OC (r = 0.325; P = 0.041). The GNI per capita and the ASMR of OC had a weak negative correlation (r = -0.088; P = 0.591) ( Figure 5 ).
ASIR and ASMR
There was a strong positive correlation between the ASIR and ASMR of OC (r = 0.824; P ≤ 0.001) ( Figure 6 ).

Discussion
According to the results of this study, among the European countries, Latvia, Bulgaria, Poland, Serbia, and Lithuania had the highest ASIR of OC and Latvia, Lithuania, Poland, Ireland, and Malta had the highest ASMR of OC. The incidence and mortality rates of OC are expected to increase between 2012 and 2035 and this increase is predicted to be more pronounced in women over 65 years of age. Moreover, our findings showed that increased HDI was associated with decreased ASIR and increased ASMR, but these relationships were not statistically significant.
According to the results of this study, European countries will have an increasing trend in OC morbidity and mortality. The morbidity and mortality caused by OC are expected to increase between 2012 and 2035 and this increase will be more significant in women over 65 years of age. In the past, the world’s population used to consist mainly of teenagers and children. However, due to the aging phenomenon (following improved life expectancy) and decreased birth rate in recent decades, older adults currently constitute a high proportion of the world’s population. With the aging of the population, an increase in the occurrence of non-communicable diseases, such as cancers, is predictable. Based on the World Health Organization (WHO) report in 2012, the aging of the population can increase the number of new cancer cases to 19.3 million in 2025. The largest rates of new cancer cases (56.8%) and deaths (64.9%) will be seen in developing countries Ferlay et al., 2013 . Cancer is estimated to be responsible for 12.6% of all deaths. While cancer is now the second cause of death, after cardiovascular diseases, worldwide, its mortality rate is expected to exceed that of cardiovascular diseases in the coming years Arab et al., 2014.
The incidence of cancer in diverse geographic areas can partly be attributed to variances in the lifestyle of their residents Rohani-Rasaf et al., 2013. The incidence of cancer can be affected by numerous factors including work-related factors, alcohol and tobacco use, food and nutrition, pollution, water pollution, infectious agents, obesity, physical activity, and ultraviolet (UV) radiation Jemal et al., 2010. Risk factors of cancer include type of nutrition, smoking, and reproductive behaviors in developed countries and infectious causes in developing countries Rohani-Rasaf et al., 2013.
One of the significant factors in decreasing cancer morbidity and mortality might be HDI, which assesses long-term advancement in three areas of human development. It is a merged index of three rudimentary dimensions of human development including life expectancy at birth, access to education (according to a combination of adult literacy rate and primary to tertiary education enrollment rates), and income (based on per capita gross domestic product adjusted for purchasing power equality in US$).
According to the results of this study, among European countries, Latvia, Bulgaria, Poland, Serbia, and Lithuania had the highest ASIR of OC. Moreover, Latvia, Lithuania, Poland, Ireland, and Malta had the highest ASMR of OC. All these countries, except for Bulgaria and Serbia, are considered to have very high human development. Evaluating the associations between HDI and the ASIR and ASMR of OC revealed that an increase in HDI decreased the ASIR and increased the ASMR of OC. Likewise, in a study on Asian countries, the relationship between HDI and the ASMR of OC was negative and not significant. However, in contrast to our findings, the results of this study showed a significant positive correlation between HDI and the ASIR of OC Razi et al., 2016.
Socioeconomic factors affect the incidence of cancer through complex and variable mechanisms. Fidler et al. reported positive correlations between HDI and the ASIR of leukemia, multiple myeloma, and lung, pancreas, gallbladder, brain/nervous system, colorectal, kidney, and thyroid cancer. Moreover, positive relations were detected between HDI and the ASIR of melanoma of the skin, Hodgkin lymphoma, and bladder, testicular, and lip/oral cavity cancers in males. HDI was also positively related with non-Hodgkin lymphoma, and breast, corpus uteri, and ovarian cancers in females. A negative correlation was detected between HDI and the ASIR of Kaposi sarcoma, and cervical and other pharyngeal cancers in females Fidler et al., 2016. Moreover, Præstegaard et al. indicated a relationship between lower level of education and an increased risk of progressive tumor stage at diagnosis of OC Præstegaard et al., 2016.
Limitation
Since this was an ecological study, its results are significant and interpretable at the population level and ecological fallacy will happen if the results are interpreted at the individual level. Some factors such as gynecological surgeries, tubal ligation, number of deliveries, gravidity, oral contraception and breastfeeding may reduce the risk of OC. On the other hand, some medical conditions and environmental factors such as endometriosis, hyperthyroidism, ovarian cysts, medical history and occupation hazards increase the risk of OC. However, in this study, we did not have access to adequate data on these factors to discuss their effects on the incidence and mortality of OC. Therefore, in addition to ecological research in each of the European countries, studies at an individual level with case-control or cohort designs are required to detect the role of factors associated with the incidence and mortality of OC at an individual level.
Conclusion
According to the results of this study, among European countries, Latvia, Bulgaria, Poland, Serbia, and Lithuania had the highest ASIR and Latvia, Lithuania, Poland, Ireland, and Malta had the highest ASMR of OC. Moreover, an increase in in HDI was associated with decreased ASIR and increased ASMR of OC. However, these relationships were not statistically significant. The morbidity and mortality of OC had an increasing trend in European countries. Therefore, it seems that health policy makers in these countries should make appropriate decisions to deal with the growth in the morbidity and mortality of OC, especially in women older than 65 years of age, in regions which may have lower access to prevention and treatment services.
Abbreviations
ASIR: Age-specific incidence rate
ASMR: Age-specific mortality rate
HDI: Human Development Index
OC: Ovarian Cancer
Author Contribution
All authors contributed to the design of the research. MM, MG, BK and HS collected the data. HS, BK and AMH conducted analysis and interpretation of data. All authors drafted the first version. MM, MA, FAB, MG, AMH edited the first draft. All authors reviewed and commented on final draft.
References
-
M.
Arab,
G.
Noghabaei,
S.N.
Kazemi.
Comparison of crude and age-specific incidence rates of breast, ovary, endometrium and cervix cancers in Iran, 2005. Asian Pacific journal of cancer prevention : APJCP.
2014;
15
:
2461-2464
.
-
F.
Bray,
A.
Jemal,
N.
Grey,
J.
Ferlay,
D.
Forman.
Global cancer transitions according to the Human Development Index (2008-2030): a population-based study. The lancet oncology.
2012;
13
:
790-801
.
-
S.
Coburn,
F.
Bray,
M.
Sherman,
B.
Trabert.
International patterns and trends in ovarian cancer incidence, overall and by histologic subtype. International Journal of Cancer.
2017
.
-
J.
Ferlay,
H.R.
Shin,
F.
Bray,
D.
Forman,
C.
Mathers,
D.M.
Parkin.
Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. International journal of cancer.
2010;
127
:
2893-2917
.
-
J.
Ferlay,
I.
Soerjomataram,
R.
Dikshit,
S.
Eser,
C.
Mathers,
M.
Rebelo,
D.M.
Parkin,
D.
Forman,
F.
Bray.
Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. International journal of cancer.
2015;
136
:
E359-E386
.
-
J.
Ferlay,
E.
Steliarova-Foucher,
J.
Lortet-Tieulent,
S.
Rosso,
J.
Coebergh,
H.
Comber,
D.
Forman,
F.
Bray.
Cancer incidence and mortality patterns in Europe: estimates for 40 countries in 2012. European journal of cancer.
2013;
49
:
1374-1403
.
-
M.M.
Fidler,
I.
Soerjomataram,
F.
Bray.
A global view on cancer incidence and national levels of the human development index. International Journal of Cancer.
2016
.
-
W.D.
Foulkes,
K.A.
Cooney.
Male Reproductive Cancers. Springer.
2010
.
-
M.
Ghoncheh,
A.
Mohammadian-Hafshejani,
H.
Salehiniya.
Incidence and mortality of breast cancer and their relationship to development in Asia. Asian Pacific journal of cancer prevention : APJCP.
2015;
16
:
6081-6087
.
-
S.
Hassanipour-Azgomi,
A.
Mohammadian-Hafshejani,
M.
Ghoncheh,
F.
Towhidi,
S.
Jamehshorani,
H.
Salehiniya.
Incidence and mortality of prostate cancer and their relationship with the Human Development Index worldwide. Prostate International.
2016
.
-
A.
Jemal,
M.M.
Center,
C.
DeSantis,
E.M.
Ward.
Global patterns of cancer incidence and mortality rates and trends. Cancer.
2010;
epidemiology
:
biomarkers & prevention : a publication of the American Association for Cancer Research, cosponsored by the American Society of Preventive Oncology 19, 1893-1907
.
-
N.
Mahdavifar,
M.
Ghoncheh,
R.
Pakzad,
Z.
Momenimovahed,
H.
Salehiniya.
Epidemiology, Incidence and Mortality of Bladder Cancer and their Relationship with the Development Index in the World. Asian Pacific journal of cancer prevention : APJCP.
2016;
17
:
381-386
.
-
M.
Mohammadian,
A.
Soroush,
A.
Mohammadian-Hafshejani,
F.
Towhidi,
F.
Hadadian,
H.
Salehiniya.
Incidence and Mortality of Liver Cancer and Their Relationship with Development in Asia. Asian Pacific journal of cancer prevention: APJCP.
2015;
17
:
2041-2047
.
-
R.
Pakzad,
A.
Mohammadian-Hafshejani,
M.
Ghoncheh,
I.
Pakzad,
H.
Salehiniya.
The incidence and mortality of lung cancer and their relationship to development in Asia. Translational lung cancer research.
2015a;
4
:
763
.
-
R.
Pakzad,
A.
Mohammadian-Hafshejani,
M.
Ghoncheh,
I.
Pakzad,
H.
Salehiniya.
The incidence and mortality of prostate cancer and its relationship with development in Asia. Prostate international.
2015b;
3
:
135-140
.
-
R.
Pakzad,
A.
Mohammadian-Hafshejani,
B.
Khosravi,
S.
Soltani,
I.
Pakzad,
M.
Mohammadian,
H.
Salehiniya,
Z.
Momenimovahed.
The incidence and mortality of esophageal cancer and their relationship to development in Asia. Annals of translational medicine.
2016;
4
.
-
C.L.
Pearce,
D.O.
Stram,
R.B.
Ness,
D.A.
Stram,
L.D.
Roman,
C.
Templeman,
A.W.
Lee,
U.
Menon,
P.A.
Fasching,
J.N.
McAlpine.
Population distribution of lifetime risk of ovarian cancer in the United States. Cancer.
2015;
epidemiology
:
biomarkers & prevention : a publication of the American Association for Cancer Research, cosponsored by the American Society of Preventive Oncology 24, 671-676
.
-
J.
Poorolajal,
E.
Jenabi,
S.Z.
Masoumi.
Body mass index effects on risk of ovarian cancer: a meta-analysis. Asian Pacific journal of cancer prevention : APJCP.
2014;
15
:
7665-7671
.
-
C.
Præstegaard,
S.K.
Kjaer,
T.S.
Nielsen,
S.M.
Jensen,
P.M.
Webb,
C.M.
Nagle,
E.
Høgdall,
H.A.
Risch,
M.A.
Rossing,
J.A.
Doherty.
The association between socioeconomic status and tumour stage at diagnosis of ovarian cancer: A pooled analysis of 18 case-control studies. Cancer epidemiology.
2016;
41
:
71-79
.
-
H.
Rafiemanesh,
A.
Mohammadian-Hafshejani,
M.
Ghoncheh,
Z.
Sepehri,
R.
Shamlou,
H.
Salehiniya,
F.
Towhidi,
B.
Makhsosi.
Incidence and Mortality of Colorectal Cancer and Relationships with the Human Development Index across the World. Asian Pacific journal of cancer prevention: APJCP.
2015;
17
:
2465-2473
.
-
S.
Razi,
M.
Ghoncheh,
A.
Mohammadian-Hafshejani,
H.
Aziznejhad,
M.
Mohammadian,
H.
Salehiniya.
The incidence and mortality of ovarian cancer and their relationship with the Human Development Index in Asia. Ecancermedicalscience.
2016;
10
:
628
.
-
S.
Razi,
H.
Rafiemanesh,
M.
Ghoncheh,
Y.
Khani,
H.
Salehiniya.
Changing Trends of Types of Skin Cancer in Iran. Asian Pacific journal of cancer prevention : APJCP.
2015;
16
:
4955-4958
.
-
M.
Rohani-Rasaf,
M.
Abdollahi,
S.
Jazayeri,
N.
Kalantari,
M.
Asadi-Lari.
Correlation of cancer incidence with diet, smoking and socio- economic position across 22 districts of Tehran in 2008. Asian Pacific journal of cancer prevention : APJCP.
2013;
14
:
1669-1676
.
-
M.
Shuja,
S.
Islamie Farsani,
H.
Salehiniya,
S.
Khazaei,
M.
Mohammadian,
M.
Aryaie,
P.
Bagheri,
F.
Allah Bakeshei,
A.
Mohammadian-Hafshejani.
Assessment the association between liver cancer incidence and mortality rate with human development index in the European countries in 2012. Biomed Res Ther.
2017
.
Comments

Downloads
Article Details
Volume & Issue : Vol 4 No 08 (2017)
Page No.: 1541-1557
Published on: 2017-08-26
Citations
Copyrights & License
This work is licensed under a Creative Commons Attribution 4.0 International License.
Search Panel
Pubmed
Google Scholar
Pubmed
Google Scholar
Pubmed
Google Scholar
Pubmed
Google Scholar
Pubmed
Google Scholar
Pubmed
Google Scholar
Pubmed
Search for this article in:
Google Scholar
Researchgate
- HTML viewed - 9474 times
- Download PDF downloaded - 2413 times
- View Article downloaded - 9 times

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}