

Diabetic foot ulcer treatment by activated platelet rich plasma: a clinical study
Copyrights: Tung Dang-Xuan Tran, Phuong Thi-Bich Le, Phuc Van Pham, 2014. License: This work is licensed under a Creative Commons Attribution 4.0 International License.
Abstract
Diabetic foot ulcer is a major complication of diabetes mellitus. It occurred in about 15% of all diabetic patients. To date, the outcome of management of diabetic foot ulcer is poor and low sufficient. Some new therapies were suggested to manage and treat this disease. In almost therapies, management of diabetic foot ulcer relates to debridement of the wound, revascularization, off-loading of the ulcer, antibacterial actions, stimulating granulation, epidermization and angiogenesis. This study aimed to evaluate the effects of activated platelet rich plasma (aPRP) on diabetic foot ulcer healing on volunteer patients. There were 6 patients enrolled in this study. All patients have non-healing foot ulcers. aPRP was isolated from peripheral blood and activated with calcium chloride. Patients were injected with aPRP two times with 14-day interval. All patients were monitored during 12 weeks. The results showed that 100% (6/6) ulcers completely closed after about 7 weeks. This result initially suggests that aPRP injection is efficient method to treat the non-healing foot ulcers. Level of evidence: IV.
Introduction
Diabetic foot ulcer is a major complication of diabetes mellitus, and is the major component of the diabetic foot. This medical condition affects to 15% of all patients with diabetes mellitus. Recent study showed that up to 88% of all lower leg amputation related to diabetic foot ulcer Alvarsson et al., 2012. More importantly the cases of diabetic mellitus patients rapidly increase to 439 million by 2030.
Diabetic neuropathy and peripheral vascular disease are 2 major factors causing diabetic foot ulcers (DFUs) Wu et al., 2007. The most difficulty of DFUs is non-healing for a long time. The main reason is related to loss of balance between metalloproteinases (MMPs) and MMP inhibitors Muller et al., 2008. This status is enhanced to become serious when combining with ischemia and vascular disease. The vascular injury and ischemia reduced the oxygen and nutrients to wound. So the wound healing mechanism cannot perform as in the non-diabetic patients. Lack of oxygen and nutrients, epithelial cells at wound can not express essential factors for healing such as VEGF and PDGF; almost of cells at wound changed metabolism and activity Lobo et al., 2013. These changes in structure and functions of cells and some factors at DFUs delayed the healing process and broke the normal healing process. Hence, when diabetic mellitus patients got DFUs, almost DFUs cannot be healed, and finally patients must be faced with lower leg amputation. In fact, DFU treatment also remains as a challenge.
At the present, DFUs were treated with some physical therapies such as vacuum-assisted closure Lone et al., 2014Nather et al., 2010Ravari et al., 2013, high-voltage pulsed current electrical stimulation Houghton et al., 2003Polak et al., 2014, hyperbaric oxygen therapy (HBOT) Kranke et al., 2012Stoekenbroek et al., 2014, negative pressure wound therapy (NPWT) Zhang et al., 2014… Some biological therapies also used in DFU treatment. Some growth factors such as EGF Singla et al.,2012Tsang et al., 2003Tuyet et al., 2009, GCSF Cruciani et al., 2013, NGF Tiaka et al., 2011, VEGF Rico et al., 2009… were evaluated in DFUs. Although these biological therapies improved the time of wound closure, these therapies had not significantly recovered wound healing. In the recent studies, scientists used a pool of growth factors from PRP Martinez-Zapata et al., 2012Saad Setta et al., 2011Villela and Santos, 2010, others used stem cells alone Blumberg et al., 2012Kirana et al.,2012Yang et al., 2013 or in combined with PRP Cervelli et al., 2009. PRP and stem cells, especially mesenchymal stem cells, could quickly heal the wounds compared to conventional therapies.
This study aimed to apply of autologous PRP in diabetic mellitus patient type 2 DFU treatment. Different to previous publication about PRP usage, in this study, diabetic mellitus patients would be injected with both PRP and PPP to improve the efficacy.
Materials – Methods
Diabetic mellitus patients
Diabetic mellitus patients type 2 have DFUs with grade I or more. These DFUs cannot heal at least 4 weeks. There were 6 patients enrolled in this study without control. All patients agreed the consent form before enrolling the study. This study approved by Ethical and Medical Committee of Van Hanh Hospital, HCM, VN. The grade of wound is recorded according to the University of Texas (grade and stage) wound classification systems Oyibo et al., 2001.
Physical examination and treatment
All patients would be done physical examination, Doppler ultrasound scan of the leg with DFUs, X-ray of the foot. Then, patients were classified to grades according to Classification of Texas University. The size of DFUs also recorded before treatment. Only patients satisfied with criteria would be collected 20 mL of peripheral blood to make PRP.
PRP preparation
20 mL of peripheral blood was used to prepare PRP and PPP according to the guideline of New-PRP Pro Kit (Geneworld Ltd., HCM, VN). Briefly, blood was centrifuged at 1.500 rpm in 5 min to obtain plasma. Then, this plasma was centrifuged at 3.500 rpm in 5 min to collect platelets as a pellet at the bottom of the centrifuge tube. Pellet was diluted in 3 mL plasma and was considered as PRP, and remaining plasma was considered as PPP. Both PRP and PPP were activated to release growth factor by Calcium chloride. When calcium chloride was added into PRP, fibrin gel was formed, and this gel was used to dress on the wound, and activated PPP was stored in -200C for using in the next days.
PRP and PPP application on DFUs
DFUs were dressed by fibrin gel in the first day. After 3 days, from day 4-8, DFUs were injected with activated PPP at the wound bed. During the treatment, diabetic mellitus patients still used antibiotics, NSAID, and vitamin. If after 2 weeks, the wound had not signs of healing, patients continued to be repeated this procedure. DFUs were examined in 12 weeks 2 weeks/time.
Results
The medical conditions of patients enrolled in this study
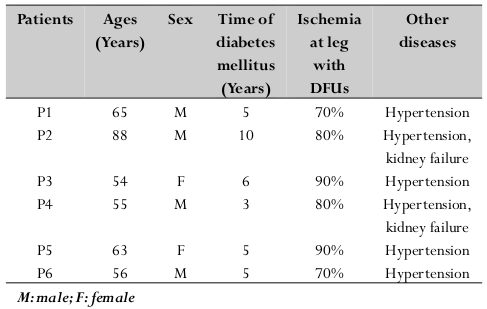
There were 6 patients with 3 males and 3 females enrolling in this study with average ages 63 with more than 5 years of diabetes mellitus. All patients must use drugs to reduce the glucose, included insulin injection, and get hypertension (4/6) and hypertension combined kidney failure (2/6). By ultrasound and X-ray, all patients received lower leg ischemia from 70-90% (artery). All patients got DFUs more than 5 weeks duration from II-III grade without granulation tissue at treatment of enrolling. The grade of wound is recorded according to the University of Texas (grade and stage) wound classification systems Oyibo et al., 2001.
Table 1 Table 1 Medical conditions of patients
Treatment efficacy
Results showed that 100% (6/6) patients completely closed the DFUs, included 2 cases with whole toes after 12 weeks. The average time for completed healing was 7.1 weeks. The soonest time was 4 weeks. All patients developed granulation tissue after 2 weeks. And wound areas significantly decreased at week 2 after one time of PRP and PPP treatment. This is the safe method to treat DFUs. During 12 weeks, there was not any adverse effect recorded in all patients ( Figure 1 ).
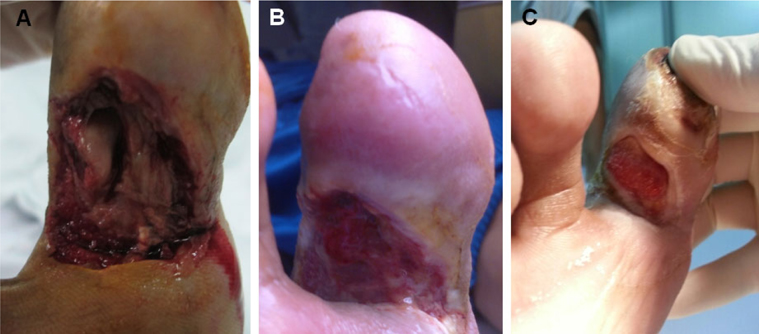
Table 2 Table 2 DFUs in patients before treatment
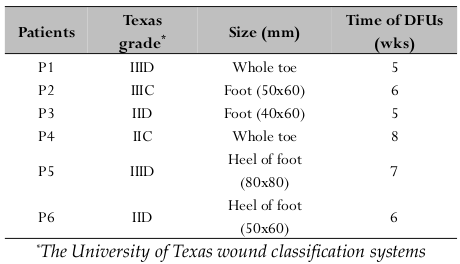
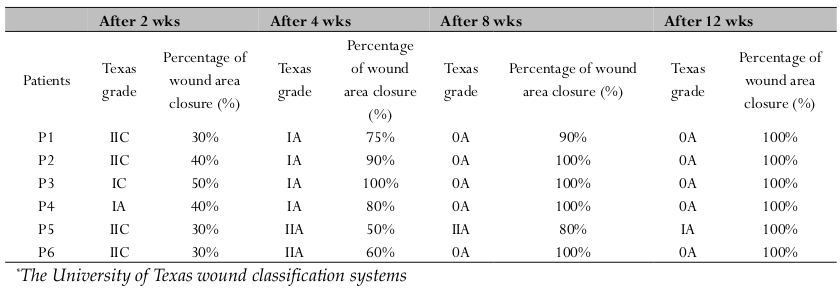
Table 3 Table 3 DFU healing after 2, 4, 8 and 12 weeks
Discussion
DFUs are results of healing process failure in diabetic mellitus patients. The lack as well as malfunction of some growth factors broke the natural healing process. PRP and PPP provided almost of growth factor for healing. In fact, all patients went to completely heal the DFUs. PRP is plasma enriched with platelets. When activated with calcium, fibrin will be formed, and platelets released growth factors. In this case, PRP exhibited two important roles for wound healing. Firstly, gel fibrin formed a barrier to prevent the bacteria contamination into the wound bed. Secondly, the growth factors from platelets triggered wound healing and balanced the wound if treated with PRP Margolis et al.,2001.
Different with our procedure, almost previous published procedure, only PRP was applied on the wound, we used both activated PRP and PPP in wound treatment. Although this study was limited with 6 patients, we also recognized that injection of activated PPP after 3 days of PRP fibrin dressing gave useful benefits to wound healing process. PPP contains very low number of platelets, but it contains a balanced pool of nutrients for cells. DFUs always combined with ischemia that significantly decreases blood flow to DFUs. All epithelial cells and support cells were starved. While PRP provides growth factors for neo-angiogenesis and cell migrations to heal the wound, PPP injection every day will provide nutrients for cells at DFUs. In fact, Saad et al. compared efficacy of PRP and PPP on wound healing in DFUs and showed that healing in PRP group was significantly faster (P<0.005) than PPP. However, PPP also well stimulated the wound healing in DFUs Saad Setta et al., 2011.
Treatment with PRP also showed that was more efficient than others. In a recent study, Lone et al. (2014) used vacuum- assisted closure method to treat DFUs. They showed that 92.85% patients developing granulation tissue by the end of 2 weeks; and 77.78% patients reached 100% granulation at the end of week 5 Lone et al., 2014.
Conclusion
DFUs seriously effected to life quality of diabetic mellitus patients. Although there are some breakthroughs in the diabetic mellitus foot care to reduce the DFUs, diabetic mellitus patients faced with amputation. In this study, in the limitation of patients, the results showed that application of PRP and PPP efficiently to heal DFUs. The results showed that there was not any adverse effect recorded in all patients during 12 weeks. These results provided a promising method for DFU treatment.
Abbreviations
bFGF: basic fibroblast growth factor; DFU: Diabetic foot ulcer; EGF: epidermal growth factor; MMPs: Metalloproteinases; MSCs: Mesenchymal stem cells; PPP: Platelet rich plasma; PRP: Platelet rich plasma; SVF: Stromal vascular fraction; VEGF: Vascular endothelial growth factor
Authors' contributions
All authors read and approved the final manuscript. TDXT, PTBL collected peripheral blood, and applied PRP and PPP on patients. PVP prepared PRP, and PPP using New-PRP Pro kit, prepared the manuscript in cooperation with all other authors.
References
-
A.
Alvarsson,
B.
Sandgren,
C.
Wendel,
M.
Alvarsson,
K.
Brismar.
A retrospective analysis of amputation rates in diabetic patients: can lower extremity amputations be further prevented?. Cardiovascular diabetology.
2012;
11
:
18
.
-
S.N.
Blumberg,
A.
Berger,
L.
Hwang,
I.
Pastar,
S.M.
Warren,
W.
Chen.
The role of stem cells in the treatment of diabetic foot ulcers. Diabetes research and clinical practice.
2012;
96
:
1-9
.
-
V.
Cervelli,
P.
Gentile,
M.G.
Scioli,
M.
Grimaldi,
C.U.
Casciani,
L.G.
Spagnoli,
A.
Orlandi.
Application of platelet-rich plasma in plastic surgery: clinical and in vitro evaluation. Tissue engineering Part.
2009;
C
:
Methods 15, 625-634
.
-
J.W.
Cho,
S.A.
Kim,
K.S.
Lee.
Platelet-rich plasma induces increased expression of G1 cell cycle regulators, type I collagen, and matrix metalloproteinase-1 in human skin fibroblasts. International journal of molecular medicine.
2012;
29
:
32-36
.
-
M.
Cruciani,
B.A.
Lipsky,
C.
Mengoli,
F.
de Lalla.
Granulocyte-colony stimulating factors as adjunctive therapy for diabetic foot infections. The Cochrane database of systematic reviews.
2013;
8
:
CD006810
.
-
P.E.
Houghton,
C.B.
Kincaid,
M.
Lovell,
K.E.
Campbell,
D.H.
Keast,
M.G.
Woodbury,
K.A.
Harris.
Effect of electrical stimulation on chronic leg ulcer size and appearance. Physical therapy.
2003;
83
:
17-28
.
-
D.H.
Kim,
Y.J.
Je,
C.D.
Kim,
Y.H.
Lee,
Y.J.
Seo,
J.H.
Lee,
Y.
Lee.
Can Platelet-rich Plasma Be Used for Skin Rejuvenation? Evaluation of Effects of Platelet-rich Plasma on Human Dermal Fibroblast. Annals of dermatology.
2011;
23
:
424-431
.
-
S.
Kirana,
B.
Stratmann,
C.
Prante,
W.
Prohaska,
H.
Koerperich,
D.
Lammers,
M.H.
Gastens,
T.
Quast,
M.
Negrean,
O.A.
Stirban.
Autologous stem cell therapy in the treatment of limb ischaemia induced chronic tissue ulcers of diabetic foot patients. International journal of clinical practice.
2012;
66
:
384-393
.
-
P.
Kranke,
M.H.
Bennett,
M.
Martyn-St James,
A.
Schnabel,
S.E.
Debus.
Hyperbaric oxygen therapy for chronic wounds. The Cochrane database of systematic reviews.
2012;
4
:
CD004123
.
-
R.
Lobo,
T.J.
Kiernan,
M.R.
Jaff.
Medical therapy for critical limb ischemia and the diabetic foot: an update. The Journal of cardiovascular surgery.
2013;
54
:
671-678
.
-
A.M.
Lone,
M.I.
Zaroo,
B.A.
Laway,
N.A.
Pala,
S.A.
Bashir,
A.
Rasool.
Vacuum-assisted closure versus conventional dressings in the management of diabetic foot ulcers: a prospective case-control study. Diabetic foot & ankle.
2014;
5
.
-
D.J.
Margolis,
J.
Kantor,
J.
Santanna,
B.L.
Strom,
J.A.
Berlin.
Effectiveness of platelet releasate for the treatment of diabetic neuropathic foot ulcers. Diabetes care.
2001;
24
:
483-488
.
-
M.J.
Martinez-Zapata,
A.J.
Marti-Carvajal,
I.
Sola,
J.A.
Exposito,
I.
Bolibar,
L.
Rodriguez,
J.
Garcia.
Autologous plateletrich plasma for treating chronic wounds. The Cochrane database of systematic reviews.
2012;
10
:
CD006899
.
-
J.P.
McAleer,
S.
Sharma,
E.M.
Kaplan,
G.
Persich.
Use of autologous platelet concentrate in a nonhealing lower extremity wound. Advances in skin & wound care.
2006;
19
:
354-363
.
-
M.
Muller,
C.
Trocme,
B.
Lardy,
F.
Morel,
S.
Halimi,
P.Y.
Benhamou.
Matrix metalloproteinases and diabetic foot ulcers: the ratio of MMP-1 to TIMP-1 is a predictor of wound healing. Diabetic medicine : a journal of the British Diabetic Association.
2008;
25
:
419-426
.
-
A.
Nather,
S.B.
Chionh,
A.Y.
Han,
P.P.
Chan,
A.
Nambiar.
Effectiveness of vacuum-assisted closure (VAC) therapy in the healing of chronic diabetic foot ulcers. Annals of the Academy of.
2010;
Medicine
:
Singapore 39, 353-358
.
-
S.O.
Oyibo,
E.B.
Jude,
I.
Tarawneh,
H.C.
Nguyen,
L.B.
Harkless,
A.J.
Boulton.
A comparison of two diabetic foot ulcer classification systems: the Wagner and the University of Texas wound classification systems. Diabetes care.
2001;
24
:
84-88
.
-
P.V.
Pham,
N.B.
Vu,
V.M.
Pham,
N.H.
Truong,
T.L.
Pham,
L.T.
Dang,
T.T.
Nguyen,
A.N.
Bui,
N.K.
Phan.
Good manufacturing practice-compliant isolation and culture of human umbilical cord blood-derived mesenchymal stem cells. Journal of translational medicine.
2014;
12
:
56
.
-
A.
Polak,
A.
Franek,
J.
Taradaj.
High-Voltage Pulsed Current Electrical Stimulation in Wound Treatment. Advances in wound care.
2014;
3
:
104-117
.
-
H.
Ravari,
M.H.
Modaghegh,
G.H.
Kazemzadeh,
H.G.
Johari,
A.M.
Vatanchi,
A.
Sangaki,
M.V.
Shahrodi.
Comparision of vacuum-asisted closure and moist wound dressing in the treatment of diabetic foot ulcers. Journal of cutaneous and aesthetic surgery.
2013;
6
:
17-20
.
-
T.
Rico,
J.
Green,
R.S.
Kirsner.
Vascular endothelial growth factor delivery via gene therapy for diabetic wounds: first steps. The Journal of investigative dermatology.
2009;
129
:
2084
.
-
H.
Saad Setta,
A.
Elshahat,
K.
Elsherbiny,
K.
Massoud,
I.
Safe.
Platelet-rich plasma versus platelet-poor plasma in the management of chronic diabetic foot ulcers: a comparative study. International wound journal.
2011;
8
:
307-312
.
-
S.
Singla,
S.
Singla,
A.
Kumar,
M.
Singla.
Role of epidermal growth factor in healing of diabetic foot ulcers. The Indian journal of surgery.
2012;
74
:
451-455
.
-
R.M.
Stoekenbroek,
T.B.
Santema,
D.A.
Legemate,
D.T.
Ubbink,
A.
van den Brink,
M.J.
Koelemay.
Hyperbaric Oxygen for the Treatment of Diabetic Foot Ulcers: A Systematic Review. European journal of vascular and endovascular surgery : the official journal of the European Society for Vascular Surgery.
2014
.
-
E.K.
Tiaka,
N.
Papanas,
A.C.
Manolakis,
E.
Maltezos.
The role of nerve growth factor in the prophylaxis and treatment of diabetic foot ulcers. International journal of burns and trauma.
2011;
1
:
68-76
.
-
M.W.
Tsang,
W.K.
Wong,
C.S.
Hung,
K.M.
Lai,
W.
Tang,
E.Y.
Cheung,
G.
Kam,
L.
Leung,
C.W.
Chan,
C.M.
Chu.
Human epidermal growth factor enhances healing of diabetic foot ulcers. Diabetes care.
2003;
26
:
1856-1861
.
-
H.L.
Tuyet,
T.T.
Nguyen Quynh,
H.
Vo Hoang Minh,
D.N.
Thi Bich,
T.
Do Dinh,
D.
Le Tan,
H.L.
Van,
T.
Le Huy,
H.
Doan Huu,
T.N.
Tran Trong.
The efficacy and safety of epidermal growth factor in treatment of diabetic foot ulcers: the preliminary results. International wound journal.
2009;
6
:
159-166
.
-
P.
Van Pham,
K.H.
Bui,
D.Q.
Ngo,
N.B.
Vu,
N.H.
Truong,
N.L.
Phan,
D.M.
Le,
T.D.
Duong,
T.D.
Nguyen,
V.T.
Le.
Activated platelet-rich plasma improves adipose-derived stem cell transplantation efficiency in injured articular cartilage. Stem cell research & therapy.
2013;
4
:
91
.
-
D.L.
Villela,
V.L.
Santos.
Evidence on the use of plateletrich plasma for diabetic ulcer: a systematic review. Growth factors.
2010;
(Chur
:
Switzerland) 28, 111-116
.
-
S.C.
Wu,
V.R.
Driver,
J.S.
Wrobel,
D.G.
Armstrong.
Foot ulcers in the diabetic patient, prevention and treatment. Vascular health and risk management.
2007;
3
:
65-76
.
-
M.
Yang,
L.
Sheng,
T.R.
Zhang,
Q.
Li.
Stem cell therapy for lower extremity diabetic ulcers: where do we stand?. BioMed research international 2013, 462179.
2013
.
-
J.
Zhang,
Z.C.
Hu,
D.
Chen,
D.
Guo,
J.Y.
Zhu,
B.
Tang.
Effectiveness and safety of negative pressure wound therapy for diabetic foot ulcers: a meta-analysis. Plastic and reconstructive surgery.
2014
.
Comments
Downloads
Article Details
Volume & Issue : Vol 1 No 02 (2014)
Page No.: 37-42
Published on: 2014-03-22
Citations
Copyrights & License
This work is licensed under a Creative Commons Attribution 4.0 International License.
Search Panel
Pubmed
Google Scholar
Pubmed
Google Scholar
Pubmed
Search for this article in:
Google Scholar
Researchgate
- HTML viewed - 8215 times
- Download PDF downloaded - 2072 times
- View Article downloaded - 19 times

{kind=link}
{kind=link}
{kind=link}
{kind=link}