

Copyrights: Naveed Akhtar, Muhammad Ilyas, Khushi Muhammad, Sulaiman Shams, Kausar Saeed, Asadullah Asadullah, 2016. License: This work is licensed under a Creative Commons Attribution 4.0 International License.
Abstract
Introduction: In the current study, prevalence of hepatitis C virus and its routes of transmission were determined in district Buner, Khyber Pakhtunkhwa, Pakistan.
Methods: Total 230 blood samples for HCV were collected from 7 tehsils of District Buner. Diaspot rapid HCV strips manufactured by Diaspot diagnostic USA were used for the detection of HCV-Ab in the blood.
Results: Out of 230 blood samples collected from patients, 158 were found positive for HCV infection. Of the 158 positive cases, 102 (64.55%) were male and 56 (35.45%) were female patients. The high rate of Hepatitis C infection was found in the age group of 41-50 years that was 68 (29.56%), followed by age group of 20-30 years that was 60 (26.08%), 31-40 years that was 54 (23.47%). The lowest infection was found in age group above 70 years.
Conclusion: It is concluded from the study that such high proportion of hepatitis C prevalence will result in high rate of mortality and morbidity in the area. Possible steps are required for the prevention and cure of such viral infections.
Introduction
Hepatitis C virus was first identified and reported in 1989. Consequent survey on the population found that hepatitis C was accountable for about 90% of all transfusion associated belongings of non–A, non-B hepatitis Aach et al., 1991Alter et al., 1989Ikeda et al., 1994.
Hepatitis “C” virus (HCV) is a spherical, enveloped, single-stranded RNA virus belonging to Flaviviridae family and genus Hepacivirus. Hepatitis “C” virus is highly heterogeneous and is classified into 11 different genotypes of which 6 are major genotypes and are further classified into many subtypes based on the genomic sequence heterogeneity. Genotypes of HCV are the intrinsic characteristics of the infecting virus strain and do not change over time Muhammad and Jan, 2005. Hepatitis “C” is an infectious disease affecting primarily the liver, caused by the hepatitis C virus (HCV). The infection is often asymptomatic, but chronic infection can lead to scarring of the liver and ultimately to cirrhosis, which is generally apparent after many years. In some cases, those with cirrhosis will go on to develop liver failure, liver cancer or life-threatening oesophageal and gastric varices Funda, 2001.
Hepatitis C virus (HCV) infection is a main global health concern. According to the world health organization, the previous worldwide burden of hepatitis C included only burden from severe HCV infectivity Organization, 2004a. Recent burden estimates shows that globally there were 54,000 deaths and 955,000 disability adjusted life-years associated with severe Hepatitis C Virus infection. Chronic sequelae infections result in Hepatitis C Virus infection Perz et al., 2006. According to the most authentic data, three to four million develop hepatitis C each year, 170 million people develop chronic infection which leads to liver disease including cirrhosis and liver cancer, and 350,000 deaths each year are due to all HCV-related causes Perz et al., 2006.
Hepatitis “C” Virus (HCV) is responsible for infecting about 170 million people globally and the second most common cause of viral hepatitis Idrees and Riazuddin, 2008. About 250,000 to 350,000 deaths occur per year because of cirrhosis, end-stage liver disease, and hepatocellular carcinoma Chevaliez and Pawlotsky, 2007 due to chronic hepatitis C infection.
Hepatitis C and Hepatitis B is responsible for morbidity and mortality and is a serious health problem globally as well as in Pakistan Ahmad et al., 2004. In Pakistan, the prevalence of hepatitis C virus infection is higher in rural areas than urban areas Aziz et al., 2010. As estimated by the Economic Survey of Pakistan, the government of Pakistan spends about 0.75 of GDP on health sector Akram, 2007. On such low provision of funds, the public sector lacks quality in its services. Pakistan had just 7.3 physicians and 4.7 nursing personnel per 1000 population Organization, 2004b.
A study was conducted in District Mardan, Khyber Pakhtunkhwa (KPK) province of Pakistan to determine the prevalence of hepatitis C virus infection. They report the overall prevalence of HCV in Mardan as 3.66%. They report the high burden of HCV in age group of 41-50 that was 7.4%. The disease burden was higher in male population that was 4.5% as compared to female population that was 2% Arshad, 2012.
A detailed study was conducted in the MMT Hospital, D I Khan and Ibrahimi Hospital and Trust, Peshawar. They reported the highest prevalence of HCV in males that was 282 (53.1%) and females 255 (46.9%). The HCV genotype details were shown as: Type 3a were 355 (66.11%), 3b were 14 (2.61%), 2a were 40 (7.45%), 2b were 5 (0.93%), type 1a were 9 (1.67%), 1b were 9 (1.67%) and patients with mixed types 2a and 3b, 3 (0.56%) were combined 3a and 3b and unable to type were 101 (18.81%) Khan et al., 2014.
The earth quake in October 2005 in Hazara Division took more than 100,000 lives and most of others were seriously injured Ahmad, 2005Sheikh, 2005. In such situation, it is feared that the transfusion of unscreened blood might have increased the risk of hepatitis C transmission Khan et al., 2003. But the fact remains that there is no accurate information available about the prevalence of hepatitis C in the area. A population based survey was conducted to estimate the prevalence of hepatitis C in the area. The accurate information regarding the prevalence of hepatitis C in the area is required to measure the shock of any interference in the area Shepard et al., 2005.
In Pakistan, the major ways of hepatitis C virus transmission are the contaminated instruments use in medical practice, unscreened blood and blood product transfusion, the uses of intravenous drugs, barber shops, piercing of ear and nose, unhygienic habits and poor medical practice by non-qualified people Ali et al., 2009aRaja and Janjua, 2008Zuberi et al., 2008. Among them, one of the major transmission route is lack of proper screening of the transfusing blood Luby et al., 1997.
According to World Health Organization, about 80% people infected with hepatitis C have no signs and symptoms Organization, 2011. The symptoms reported in 20-30% of people recently infected with hepatitis C are tiredness, abdominal pain, poor appetite, or jaundice Prevention, 2012.
The result of antibodies to various viral antigens shows infection with the virus and in most cases portrays a constant infection Mc Lean, 1997. The duration of hepatitis C might be extended and dangerous and the patients with hepatitis C will develop no sign and symptoms for many years after the inception of infection Mc Lean, 1997.
Majority of the studies conducted are based on hospitalised patient data due to which true prevalence of HCV infection could not be determined. So far, no population based study has been conducted to investigate the prevalence of active HCV infection or anti-HCV antibodies in district Buner. This study aims to determine the prevalence of anti-HCV antibodies and HCV infection in the general population of district Buner.
Methods
Introduction to District Buner
District Buner is situated between 34°-11’ and 34°-43’ North - Latitude and 72°-13’ and 72°- 45’ East _ Longitude in Khyber Pakhtunkhwa province of Pakistan. The District is surrounded by Swat district on North, Malakand Agency on the West Mardan district on the South and Hazara Division on the east having altitudinal range 366-291 m, with a total area of 1865 km2 and population of 506,048 individuals Khan et al., 2012 ( Figure 1 ).
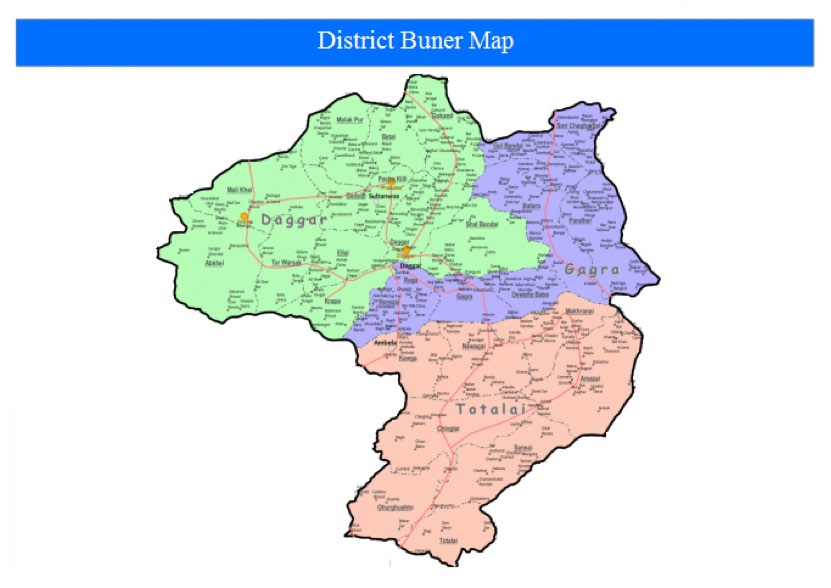
District is subdivided into 7 tehsils, namely
1.Tehsil Daggar.
2.Tehsil Gagra.
3. Tehsil Gadezai.
4.Tehsil Mandar.
5.Tehsil Chagharzi.
6.Tehsil Amazi.
7. Tehsil Khodo Khel.
Samples collection
During this study, two hundred and thirty blood samples were collected from the seven tehsils of district Buner, Khyber Pakhtunkhwa, Pakistan. The collection was done through specialised proforma which will contain the whole information about the patient. After completing the initial data, 3 mL blood was collected through (Shifa) disposable syringes. The collected blood was then transferred to serum tubes (ATLAS-LABOVAC Italiano) containing oxalate to minimise the chance of blood clotting. The blood was then transferred to the Human Genetics Lab of Hazara University, Mansehra. The blood was then centrifuged to separate serum. The separated serum was then transferred to Eppendorf tubes and was stored at -80oC.
Assay for detection of HCV Antibody
The strips used for the detection of HBsAg in the blood were DiaSpot® HCV-Ab Test strips (manufactured by DiaSpot Diagnostics, USA), Global® HCV-Ab Kit (manufactured by Global Diagnostics, USA). These methods are immunochromatographic and qualitative in nature and identify the presence of HBsAg in human blood and might interpret in vitro having more than 99.9% sensitivity and 98.6% specificity. The manufacturer’s specifications were followed to perform the test.
Approval from ethical community
The research was approved from the ethical community of district Buner.
Results
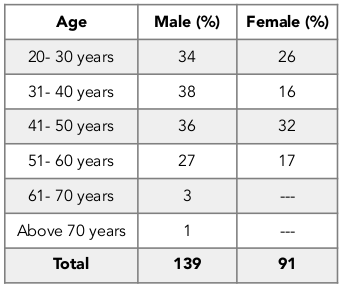
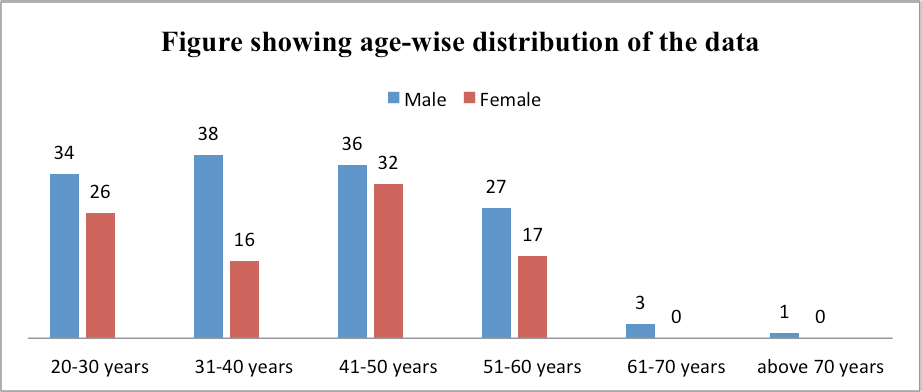
A descriptive study was conducted to find out the prevalence of HCV infection in the general population of district Buner, Khyber Pakhtunkhwa, Pakistan. In this study, 230 blood samples were collected from the whole district Buner along with the proforma for taking whole information from the patient. Among the total 230 blood samples, 139 were males and 91 were females. The data was collected from different age groups. The infection rate was different in different age groups. The details are given in Table 1 and Figure 2 .
Signs and symptoms
During the study, patients were interviewed about the HCV. The signs and symptoms of the patients were recorded on the designed proforma. The patients were showing different signs and symptoms. Fatigue was common in all patients that was 100%, joint pain was also common and was 100%, redness on the palm of hands was 100%, damage to brain and nervous system was 90.50%, belly pain was 75.94%, sore muscles was 74.68%, jaundice was 72.78%, itchy skin was 56.96%, shrinking of muscles was 29.11%, cluster of blood vessels below skin was 23.41%, swelling of belly, legs, feet was 14.56%, dark urine was 4.43%, bleeding from enlarged veins in digestive tract was 0%. The details of signs and symptoms of HCV are given in Table 2 .

Routes of transmission
In this study, the routes of transmission of hepatitis C were determined. The major ones contributing for hepatitis C in District Buner were Intravenous Drug Users (IDUs), Blood transfusion (BT), surgery, dialysis, GYN wards, barber shops, piercing in unclean environment and unsafe sex.
Discussion
Hepatitis is a public health problem worldwide. Infectious diseases including Hepatitis C are major health issues in various developing countries including Pakistan Ali et al., 2009aKhan and Siddiqui, 2007. According to an estimate of the World Health Organization, hepatitis C has effected almost 3% population of the world, an estimate of 170 million people, with an increase in three to four million new cases every year Raza et al., 2007.
In current study, we attempt to investigate the prevalence of hepatitis C virus infection and its modes of transmission in district Buner, Khyber Pakhtunkhwa, Pakistan. In current study, we collected 230 samples from whole Buner district in which 158 were positive and 72 were found negative for HCV infection.
A study conducted by Huda et al (2013) showed that the infection rate of hepatitis C virus was high in males that was 20% while in females it was 13.33% ul Huda et al., 2013. A study conducted by Arshad et al (2012) reported high prevalence of hepatitis C in male population that was 4.5% compared to females that was 2% Arshad, 2012. According to Ilyas et al (2011), the rate of HCV infection was higher in males as compared to females that was 2.60% and 1.68% respectively Ilyas et al., 2011. Other studies conducted in Pakistan also shows the higher frequency of Hepatitis C in males as compared to females Khan and Siddiqui, 2007Khan et al., 2003Mashud, 2004. The reason behind high prevalence of Hepatitis C infection in males might be freedom and social mobility in which there is high risk of contracting viral infection. In our study, the total number of 230 samples were collected in which 158 samples were positive. In these 158 samples, 102 were males and 56 were females. Our result is supported by the previous results in which the rate of incidence of hepatitis C is higher in males than that of females.
According to Ahmad et al (2004), hepatitis C and hepatitis B have high prevalence in age group of 55-64 years and low in the age group of 25-34 years Ahmad et al., 2004. Arshad et al (2012) reported highest prevalence of HCV in age group 41-50 that was 7.4%, followed by age group 51 and above that was 6.36% Arshad, 2012. Different age groups and many other factors are associated with prevalence of Hepatitis C virus infection in different regions of Pakistan Khan et al., 2011. In our study, the high rate of Hepatitis C infection was found in the age group of 41-50 years that was 68 (29.56%), followed by age group of 20-30 years that was 60 (26.08), 31-40 years that was 54 (23.47%) while the lowest infection was found in age group of above 70 years that was 1 (0.43).
According to Adeyemi et al (2014), blood transfusion is one of the major route of viral hepatitis. The false negative results in the blood banking results in the transfusion of infected blood to an uninfected person Adeyemi et al., 2014. There is an important role of blood transfusion in the epidemiology of HCV infection Bialek and Terrault, 2006. Study on blood donors in Kathmandu, Nepal results in 0.64% seroprevalence of HCV Shrestha et al., 2009. Imoru et al (2003) reported 0.4 % prevalence of hepatitis C virus antibody in Kano State Imoru et al., 2003. The unscreened blood products are one of the leading causes of hepatitis C virus transmission. The incidence of post-transfusion of hepatitis C in United States has dropped from 3.84% to 0.57% after the introduction of HCV screening in 1990 Donahue et al., 1992. In our study, blood transfusion was one of the route for hepatitis C virus infection. In previous literatures, the prevalence of HCV in the blood donors has showed lower, but we cannot neglect the risk of transmission of HCV through blood and its products.
Contaminated surgical instruments, contaminated needles and syringes are one of the important source of HCV transmission globally Hauri et al., 2004Luby et al., 1997. Developing countries have the higher risk of incidence of HCV than developed countries Bialek and Terrault, 2006. Egypt has the highest rate of hepatitis C incidence that is five-fold than in developed countries Strickland, 2006. HCV can transmit from infected patients to health workers through needle injuries with the infection rate about 1.8% Beltrami et al., 2000. The higher rate of infection had been reported in the dialysis patients. Saudi Arabia had showed the high rate of prevalence in the haemodialysis patients that is 9.24% as that of blood donors that is 0.30% Qadi et al., 2004. These studies show the transmission of hepatitis C through haemodialysis patients due to poor sterile techniques, poor cleaning of dialysis machine and other possible ways increase the risk of hepatitis C transmission among the patients Zampieron et al., 2004.
Intravenous drug usage is the prominent mode of transmission of hepatitis C virus in the developed countries. In USA, the incidence of hepatitis C cases increased from 31% in 1994 to 38% in 1999 and reached to 45% in 2003 Prevention, 2005.
Among the 310 drug users in Antwerp, prevalence of anti-HCV antibody was 71% and in Limburg in Belgium was 46% Matheï et al., 2005. The Hepatitis C European Network for C-operative Research (HENCORE) group had reported the prevalence of 80% hepatitis C among intravenous drug users (IVDU) Touzet et al., 2000. There was 36.6% positivity of hepatitis C in the intravenous drug users in Sydney, Australia and 74% hepatitis C positivity in the intravenous drug users in Melbourne, Australia Bradshaw et al., 2005Maher et al., 2004. In the recent study in London, England, the 428 intravenous drug users were under the age of 30 having 44% antibodies to hepatitis C compared to 4% with HIV, this is the incidence of 41.8 cases per 100 persons Judd et al., 2004. Most of such patients are not aware from the risk of transmission and sometimes they do not know that they are infected, therefore screening of such group is important.
In a study, conducted by Ali et al (2009b) the major symptoms of hepatitis C virus were high bilirubin with high liver enzymes that was 17.94%, yellowish eyes with skin colouration was 15.39% and dark yellow urine with diarrhoea was 10.25%, fever was 15.38%, vomiting was 12.82%, loss of appetite was 7.69%, stomach pain was 5.12% and tiredness was 2.56%. They also reported that 56.41% patients were infected with HCV, but were presenting no symptoms Ali et al., 2009b. During our study, the patients were showing different signs and symptoms. Fatigue was common in all patients that was 100%, joint pain was also common and was 100%, redness of the palm of hands was 100%, damage to brain and nervous system was 90.50%, belly pain was 75.94%, sore muscles was 74.68%, jaundice was 72.78%, itchy skin was 56.96%, shrinking of muscles was 29.11%, cluster of blood vessels below skin was 23.41%, swelling of belly, legs, feet was 14.56%, dark urine was 4.43%, bleeding from enlarged veins in digestive tract was 0%.
Approximately, 30% of health care workers having hepatitis C infection was reported from one of the teaching hospital at Abbottabad, Pakistan Sarwar et al., 2007. Along with this, the unclean dental equipment is common in almost every dental clinic of Pakistan Ali et al., 2009a. In our study, it was found that most of the people infected with hepatitis C were health care workers because they have a higher risk of getting hepatitis C virus through contact with the blood and blood products of the patients.
One of the most common factors associated with the transmission of hepatitis C is the disposal of hospital waste Riaz et al., 2012. There are hundreds of garbage collectors of different age groups throughout the country who are associated with main recycling businessmen who deal unsterile syringes. The young scavenger in Karachi, Pakistan of about 18 to 20 years of age sells 20 to 25 syringes per day to the health care waste dealers and with these needles the same child gets injured around none to three times per week Mujeeb et al., 2003. In our study, it was found that most of the children between the age of 12 to 18 years regularly collect the waste like syringes and other plastic materials from the hospitals and other health care providers and sell them to scrape dealers for money. During this collection, some of the needles pierce into their fingers and feet and injure them. During these injuries, there is a higher chance of developing diseases such as hepatitis C.
Hepatitis C virus (HCV) infection has become one of the most important public health concern round the globe Costa et al., 2009. Pakistan is also facing a huge burden of these diseases. The prevalence among general public of HBV and HCV infection in Pakistan is 10% Malik et al., 1996Yousaf et al., 1996 and 4–10% respectively Malik et al., 1996Umar et al., 2000. In our study, it was found that hepatitis C is the major health problem in district Buner. Data from the whole district was collected which shows that hepatitis C is prevalent in district Buner and if the protective measures are not adopted, then it is possible that hepatitis C will become one of the major health problem in district Buner, Khyber Pakhtunkhwa, Pakistan.
Conclusion
Hepatitis C is widely prevalent in district Buner, Khyber Pakhtunkhwa, Pakistan. Such high proportion of hepatitis C prevalence will result in the high rate of mortality and morbidity in the area; therefore, possible steps are required for the prevention and cure of such viral infections. It is concluded that for the development of appropriate vaccines, research at the molecular level is required to understand the predominant genotypes circulating in district Buner, Khyber Pakhtunkhwa, Pakistan.
List of Abbreviations
HCV: Hepatitis C Virus
HENCORE: Hepatitis C European Network for C-operative Research IVDU: Intravenous Drug Users
ml: Milliliter
USA: United State of America WHO: World Health Origination KPK: Khyber Pakhtunkhwa
KM: Kilometer
Ethical Approval
The research was approved from the ethical community of district Buner.
Authors’ contributions
NA carried out this prevalence study. He collected the samples and got the consent of subjects. HA, KM and SS mainly supervised this study. NA, KM and KS prepared the manuscript. All authors read and approved the final manuscript.
References
-
R.D.
Aach,
C.E.
Stevens,
F.B.
Hollinger,
J.W.
Mosley,
D.A.
Peterson,
P.E.
Taylor,
R.G.
Johnson,
L.H.
Barbosa,
G.J.
Nemo.
Hepatitis C virus infection in post-transfusion hepatitis: an analysis with first-and second-generation assays. New England Journal of Medicine.
1991;
325
:
1325-1329
.
-
A.
Adeyemi,
O.
Omolade,
R.
Raheem-Ademola.
Immunochromatographic testing method for hepatitis B, C in blood donors. Journal of Antivirals & Antiretrovirals 2014.
2014
.
-
I.
Ahmad,
S.B.
Khan,
H.
ur Rehman,
M.H.
Khan,
S.
Anwar.
Frequency of Hepatitis B and Hepatitis C among cataract patients. Gomal Journal of Medical Sciences.
2004;
4
.
-
K.
Ahmad.
Quake victims reach help too late to save crushed limbs. Bulletin of the World Health Organization.
2005;
83
:
889-891
.
-
M.
Akram,
F.J.
Khan.
Health care services and government spending in Pakistan. Pakistan iinstitute of development economics.
2007
.
-
M.
Ali,
L.
Kanwal,
K.
Tassaduqe,
R.
Iqbal.
Prevalence of hepatitis C virus (HCV) in relation to its promotive factors among human urban population of Multan, Pakistan. European Journal of General Medicine.
2009a;
6
.
-
S.A.
Ali,
R.M.
Donahue,
H.
Qureshi,
S.H.
Vermund.
Hepatitis B and hepatitis C in Pakistan: prevalence and risk factors. International journal of infectious diseases.
2009b;
13
:
9-19
.
-
M.J.
Alter,
P.J.
Coleman,
W.J.
Alexander,
E.
Kramer,
J.K.
Miller,
E.
Mandel,
S.C.
Hadler,
H.S.
Margolis.
Importance of heterosexual activity in the transmission of hepatitis B and non-A, non-B hepatitis. Jama.
1989;
262
:
1201-1205
.
-
A.
Arshad,
M.
Arshad,
R.
Pervaiz,
Javed
Farzana,
N.
Ahmad,
I. Saljoqi
Ali.
Prevalance of active Hepatitis-C infection in the general population of District Mardan, Khyber Pakhtunkhwa, Pakistan. Journal of Public Health and Biological Sciences.
2012;
1
:
3-8
.
-
S.
Aziz,
R.
Khanani,
W.
Noorulain,
J.
Rajper.
Frequency of hepatitis B and C in rural and periurban Sindh. JPMA-Journal of the Pakistan Medical Association.
2010;
60
:
853
.
-
E.M.
Beltrami,
I.T.
Williams,
C.N.
Shapiro,
M.E.
Chamberland.
Risk and management of blood-borne infections in health care workers. Clinical microbiology reviews.
2000;
13
:
385-407
.
-
S.R.
Bialek,
N.A.
Terrault.
The changing epidemiology and natural history of hepatitis C virus infection. Clinics in liver disease.
2006;
10
:
697-715
.
-
C.
Bradshaw,
L.
Pierce,
S.
Tabrizi,
C.
Fairley,
S.
Garland.
Screening injecting drug users for sexually transmitted infections and blood borne viruses using street outreach and self collected sampling. Sexually Transmitted Infections.
2005;
81
:
53-58
.
-
S.
Chevaliez,
J.-M.
Pawlotsky.
Hepatitis C virus: virology, diagnosis and management of antiviral therapy. World journal of gastroenterology.
2007;
13
:
2461
.
-
Z.B.
Costa,
G.C.
Machado,
M.M.
Avelino,
C.
Gomes Filho,
J.V.
Macedo Filho,
A.L.
Minuzzi,
M.D.
Turchi,
M.M.
Stefani,
W.V.
de Souza,
C.M.
Martelli.
Prevalence and risk factors for Hepatitis C and HIV-1 infections among pregnant women in Central Brazil. BMC infectious diseases.
2009;
9
:
1
.
-
J.G.
Donahue,
A.
Muñoz,
P.M.
Ness,
D.E.
Brown Jr,
D.H.
Yawn,
H.A.
McAllister Jr,
B.A.
Reitz,
K.E.
Nelson.
The declining risk of post-transfusion hepatitis C virus infection. New England journal of medicine.
1992;
327
:
369-373
.
-
S.
Funda.
Identification of predominant Hepatitis “C” virus genotype in Turkish population. In Deptt of molecular biology & Genetics Bilkent (University Turkey).
2001
.
-
A.M.
Hauri,
G.L.
Armstrong,
Y.J.
Hutin.
The global burden of disease attributable to contaminated injections given in health care settings. International journal of STD & AIDS.
2004;
15
:
7-16
.
-
M.
Idrees,
S.
Riazuddin.
Frequency distribution of hepatitis C virus genotypes in different geographical regions of Pakistan and their possible routes of transmission. BMC infectious diseases.
2008;
8
:
1
.
-
Y.
Ikeda,
H.
Nakano,
T.
Sakemi,
Y.
Nagano,
N.
Otsuka,
N.
Baba,
Y.
Syouno,
K.
Yamaguchi.
[A case of membranoproliferative glomerulonephritis due to type II cryoglobulinemia probably associated with hepatitis C virus infection]. Nihon Jinzo Gakkai shi.
1994;
36
:
284-288
.
-
M.
Ilyas,
M.
Iftikhar,
U.
Rasheed.
Prevalence of hepatitis B and hepatitis C in populations of college students in Gujranwala. Biologia (Pakistan).
2011;
57
:
89-95
.
-
M.
Imoru,
C.
Eke,
A.
Adegoke.
Prevalence of Hepatitis-B Surface Antigen (HbsAg), Hepatitis C Virus (HCV) and Human Immunodeficiency Virus (HIV) among Blood Donors in Kano State, Nigeria. Journal of Medical Laboratory Science.
2003;
12
:
59-63
.
-
A.
Judd,
M.
Hickman,
S.
Jones,
T.
McDonald,
J.V.
Parry,
G.V.
Stimson,
A.J.
Hall.
Incidence of hepatitis C virus and HIV among new injecting drug users in London: prospective cohort study. Bmj.
2004;
330
:
24-25
.
-
A.J.
Khan,
T.R.
Siddiqui.
Prevalence and importance of hepatitis B and C screening in cases undergoing elective eye surgery. Pak J Ophthalmol.
2007;
23
.
-
N.U.
Khan,
I.
Ali,
N.U.
Ahmad,
A.
Iqbal,
L.U.
Rehman,
I.
Munir,
M.U.
Rehman,
S.
Khan,
S.
Ali,
L.
Siddique.
Prevalence of active HCV infection among the blood donors of Khyber Pakhtunkwa and FATA region of Pakistan and evaluation of the screening tests for anti-HCV. Virology journal.
2011;
8
:
1
.
-
S.
Khan,
F.
Haq,
K.
Saeed.
Pollution load in industrial effluent and ground water due to marble industries in District Buner, Khyber Pakhtunkhwa, Pakistan. International Journal of Recent Scientific Research.
2012;
3
:
366-368
.
-
T.M.
Khan,
M.T.
Mehr,
H.
Ullah,
H.
Khan,
N.U.
Iman.
Frequency of hepatitis C virus genotypes in the north of Pakistan. Gomal Journal of Medical Sciences.
2014;
12
.
-
T.S.
Khan,
F.
Rizvi,
A.
Rashid.
Hepatitis C seropositivity among chronic liver disease patients in Hazara, Pakistan. J Ayub Med Coll Abbottabad.
2003;
15
:
53-55
.
-
S.
Luby,
K.
Qamruddin,
A.
Shah,
A.
Omair,
O.
Pahsa,
A.
Khan,
J.
McCormick,
F.
Hoodbhouy,
S.
Fisher-Hoch.
The relationship between therapeutic injections and high prevalence of hepatitis C infection in Hafizabad, Pakistan. Epidemiology and infection.
1997;
119
:
349-356
.
-
L.
Maher,
K.
Chant,
B.
Jalaludin,
P.
Sargent.
Risk behaviors and antibody hepatitis B and C prevalence among injecting drug users in south-western Sydney, Australia. Journal of gastroenterology and hepatology.
2004;
19
:
1114-1120
.
-
A.
Malik,
S.
Butt,
W.
Tariq.
Hepatitis C virus in perspective, where do we stand [editorial]. J Coll Physician Surg Pak.
1996;
6
:
136
.
-
I.
Mashud.
Relative Frequency of Hepatitis B and Hepatitis C viruses in patients with Hepatic Cirrhosis at DHQ Teaching Hospital DI Khan. J Ayub Med Coll Abbottabad.
2004;
15
:
32-34
.
-
C.
Matheï,
G.
Robaeys,
P.
Van Damme,
F.
Buntinx,
R.
Verrando.
Prevalence of hepatitis C in drug users in Flanders: determinants and geographic differences. Epidemiology and infection.
2005;
133
:
127-136
.
-
F.M.
Mc Lean,
P. Peutherer
Morgan; Copner.
Arboviruses. In Medical microbiology, R.C.B.S. D. Greenwood, J.F., Peutherer, ed. (Livingstone).
1997
.
-
N.
Muhammad,
M.A.
Jan.
Frequency of hepatitis" C" in Buner, NWFP. Journal of the College of Physicians and Surgeons--Pakistan: JCPSP.
2005;
15
:
11-14
.
-
S.A.
Mujeeb,
M.M.
Adil,
A.
Altaf,
Y.
Hutin,
S.
Luby.
Recycling of injection equipment in Pakistan. Infection Control & Hospital Epidemiology.
2003;
24
:
145-146
.
-
W.H.
Organization.
Global burden of disease (GBD) for hepatitis C. J Clin Pharmacol.
2004a;
44
:
20-29
.
-
W.H.
Organization.
WHO-Regional Office for the Eastern Meditterranean. Country profiles-Pakistan. Retrieved October, 5, 2009.
2004b
.
-
W.H.
Organization.
Hepatitis C. World Health Organization.
2011
.
-
J.F.
Perz,
G.L.
Armstrong,
L.A.
Farrington,
Y.J.
Hutin,
B.P.
Bell.
The contributions of hepatitis B virus and hepatitis C virus infections to cirrhosis and primary liver cancer worldwide. Journal of hepatology.
2006;
45
:
529-538
.
-
C.f.D.C.a.
Prevention.
Hepatitis surveillance report. Atlanta (GA). US. Department of Health and Human Services.
2005
.
-
C.f.D.C.a.
Prevention.
Hepatitis C FAQs for Health Professionals. 2012
.
-
A.A.
Qadi,
H.
Tamim,
G.
Ameen,
A.
Bu-Ali,
S.
Al-Arrayed,
N.A.
Fawaz,
W.Y.
Almawi.
Hepatitis B and hepatitis C virus prevalence among dialysis patients in Bahrain and Saudi Arabia: a survey by serologic and molecular methods. American journal of infection control.
2004;
32
:
493-495
.
-
N.S.
Raja,
K.A.
Janjua.
Epidemiology of hepatitis C virus infection in Pakistan. Journal of Microbiology Immunology and Infection.
2008;
41
:
4
.
-
S.
Raza,
G.
Clifford,
S.
Franceschi.
Worldwide variation in the relative importance of hepatitis B and hepatitis C viruses in hepatocellular carcinoma: a systematic review. British journal of cancer.
2007;
96
:
1127-1134
.
-
H.
Riaz,
S.W.
Kamal,
T.
Riaz,
S.
Aziz,
J.
Rajper,
W.
Noorulain.
Methods of disposal of used syringes by hepatitis B and C patients at an urban and rural setting. JPMA The Journal of the Pakistan Medical Association.
2012;
62
:
81-84
.
-
J.
Sarwar,
N.
Gul,
M.
Idris,
J.
Farid,
M.
Adeel.
Seroprevalence of hepatitis B and hepatitis C in health care workers in Abbottabad. Journal of Ayub Medical.
2007;
College
:
Abbottabad: JAMC 20, 27-29
.
-
M.
Sheikh.
Earthquake in Northern Pakistan and AJK. Journal of the College of Physicians and Surgeons--Pakistan: JCPSP.
2005;
15
:
747
.
-
C.W.
Shepard,
L.
Finelli,
M.J.
Alter.
Global epidemiology of hepatitis C virus infection. The Lancet infectious diseases.
2005;
5
:
558-567
.
-
A.C.
Shrestha,
P.
Ghimire,
B.R.
Tiwari,
M.
Rajkarnikar.
Transfusion-transmissible infections among blood donors in Kathmandu, Nepal. The Journal of Infection in Developing Countries.
2009;
3
:
794-797
.
-
G.T.
Strickland.
Liver disease in Egypt: hepatitis C superseded schistosomiasis as a result of iatrogenic and biological factors. Hepatology.
2006;
43
:
915-922
.
-
S.
Touzet,
L.
Kraemer,
C.
Colin,
P.
Pradat,
D.
Lanoir,
F.
Bailly,
R.C.
Coppola,
S.
Sauleda,
M.R.
Thursz,
H.
Tillmann.
Epidemiology of hepatitis C virus infection in seven European Union countries: a critical analysis of the literature. European journal of gastroenterology & hepatology.
2000;
12
:
667-678
.
-
W.
Huda,
N.
Jameel,
U.
Fasih,
A.
Rehman,
A.
Shaikh.
Prevalence of Hepatitis B and C in Urban Patients Undergoing Cataract Surgery. Pakistan Journal of Ophthalmology.
2013;
29
:
147
.
-
M.
Umar,
A.
Shuaib,
A.
Anwar,
N.
Shah.
Spectrum of chronic liver disease due to hepatitis" C" virus infection. JCPSP; Journal of the College of Physicians and Surgeons Pakistan.
2000;
10
:
380-383
.
-
A.
Yousaf,
A.
Mohammad,
M.
Ishaque,
M.
Yousaf.
Can we afford to operate on patients without HBs Ag screening. J Coll Phys Surg Pak.
1996;
9
:
98-100
.
-
A.
Zampieron,
H.
Jayasekera,
M.
Elseviers,
E.
Lindley,
J.Y.
DeVos,
R.
Visser,
M.
Harrington.
European study on epidemiology and the management of HCV in the haemodialysis population. Part 1: Centre policy. Edtna-Erca Journal.
2004;
30
:
84-90
.
-
B.F.
Zuberi,
F.F.
Zuberi,
A.
Vasvani,
N.
Faisal,
S.
Afsar,
J.
Rehman,
B.
Qamar,
B.
Jaffery.
Appraisal of the knowledge of Internet users of Pakistan regarding hepatitis using on-line survey. J Ayub Med Coll Abbottabad.
2008;
20
:
91-93
.
Comments
Downloads
Article Details
Volume & Issue : Vol 3 No 12 (2016)
Page No.: 1003-1017
Published on: 2016-12-02
Citations
Copyrights & License
This work is licensed under a Creative Commons Attribution 4.0 International License.
Search Panel
Pubmed
Google Scholar
Pubmed
Google Scholar
Pubmed
Google Scholar
Pubmed
Google Scholar
Pubmed
Google Scholar
Pubmed
Search for this article in:
Google Scholar
Researchgate
- HTML viewed - 8088 times
- Download PDF downloaded - 2798 times
- View Article downloaded - 69 times

{kind=link}
{kind=link}
{kind=link}
{kind=link}