

Late-Onset Congenital Diaphragmatic Hernia in Adults with Normal Karyotype: Case-Based Experience from a Tertiary Center
- Department of Gastrosurgery Apollo Clinic, Gurugram, Haryana, India
- Department of Pathology, AIIMS Kalyani, West Bengal, India
- Department of Anatomy, AIIMS Kalyani, West Bengal, India
Abstract
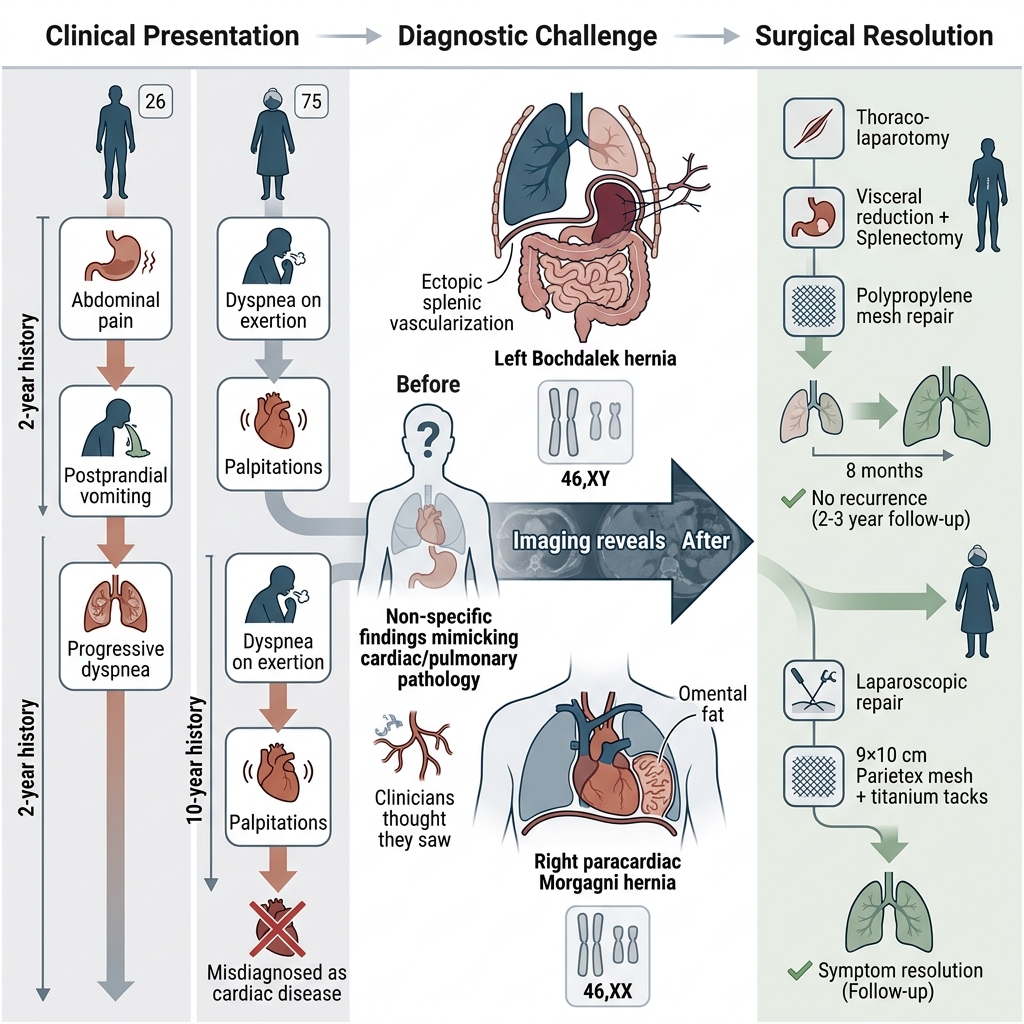
Background: Congenital diaphragmatic hernia (CDH) is predominantly diagnosed in the neonatal period due to severe respiratory compromise. Adult-onset or late-presenting CDH is rare and poses a significant diagnostic challenge due to its highly variable and nonspecific clinical manifestations. While chromosomal abnormalities are well-characterized in neonatal populations, their prevalence and genetic landscape in adult-presenting CDH remain scarcely investigated.
Case Presentation: We report two cases of late-presenting CDH in previously healthy adult patients who initially exhibited nonspecific gastrointestinal and respiratory symptoms. These ambiguous clinical manifestations led to primary consultations with cardiologists and subsequent misdiagnoses, consequently delaying appropriate management. Definitive diagnosis was established through radiological imaging, including chest radiography and computed tomography (CT), which revealed intrathoracic herniation of abdominal contents. Both patients underwent successful surgical correction involving visceral reduction and prosthetic mesh repair of the diaphragmatic defect. The postoperative courses were uneventful, resulting in complete clinical recovery. Cytogenetic analysis via conventional karyotyping demonstrated normal chromosomal patterns (46,XY and 46,XX), indicating that both cases represented isolated, non-syndromic forms of CDH.
Conclusion: Adult CDH is frequently misdiagnosed due to atypical, masquerading presentations. While conventional karyotyping remains a reasonable initial step to exclude gross numerical aberrations, advanced molecular techniques, such as chromosomal microarray analysis (CMA), provide a higher diagnostic yield when a genetic etiology is strongly suspected.
Introduction
Congenital diaphragmatic hernia (CDH), although primarily diagnosed in the neonatal period, can occasionally manifest later in life, an entity referred to as late-presenting or adult CDH. Initially described by Lazarus Riverius in 1690 during the autopsy of a 24-year-old male, adult CDH remains a rare and underdiagnosed entity 1. Pathophysiologically, it results from a developmental defect in the diaphragm—most frequently a Bochdalek hernia—which permits the herniation of abdominal contents into the thoracic cavity. Unlike the neonatal presentation, which is typically characterized by severe respiratory distress, adult cases frequently manifest with nonspecific gastrointestinal or cardiopulmonary symptoms, including chest pain, dyspnea, vomiting, epigastric fullness, or clinical features masquerading as myocardial infarction or gastroesophageal reflux disease 2,3.
Within the context of the Indian healthcare setting, this condition assumes heightened clinical relevance. Patients often bypass primary care pathways, presenting directly to cardiologists or emergency departments with distressing thoracic symptoms. In such scenarios, absent a comprehensive initial clinical evaluation or diagnostic imaging, CDH may be misdiagnosed as more common conditions, such as acute coronary syndrome, pulmonary embolism, or acute gastrointestinal disorders 4,5. Consequently, diagnostic delays and misdiagnoses are common, potentially leading to inappropriate therapeutic interventions, ranging from unnecessary antiplatelet therapy to invasive cardiac evaluations, thereby risking a critical delay in mandatory surgical intervention.
Moreover, access to advanced imaging modalities, such as computed tomography (CT) or magnetic resonance imaging (MRI), is limited in many peripheral or rural hospitals across India, where plain chest radiography remains the primary diagnostic tool. In the absence of a high index of clinical suspicion, radiological findings suggestive of CDH—such as the presence of intrathoracic bowel loops—may be misinterpreted, especially in emergency settings 6.
Therefore, enhanced awareness and clinical vigilance regarding adult CDH among physicians—especially cardiologists and emergency care providers—is crucial to prevent misdiagnoses and optimize patient outcomes. Given the demographic and unique healthcare-seeking behaviors within the Indian population, where atypical clinical profiles are prevalent, recognizing CDH in the differential diagnosis of patients with unexplained chest or abdominal symptoms is vital.
Case 1
A 26-year-old male presented with a two-year history of intermittent upper abdominal pain, along with episodes of postprandial vomiting and dyspnea, which were particularly exacerbated immediately following food intake. The symptoms followed a waxing and waning course but had progressively increased in frequency and intensity over the preceding few months, significantly impacting the patient's quality of life. There was no prior history of trauma, previous surgical interventions, or chronic illnesses. The patient reported no history of weight loss, fever, or jaundice, and exhibited normal bowel and bladder habits. On general physical examination, the patient was afebrile and hemodynamically stable, with no evidence of pallor, icterus, cyanosis, clubbing, or lymphadenopathy. His respiratory rate was mildly elevated at 22 breaths per minute.
On abdominal examination, the abdomen appeared scaphoid and was non-tender upon palpation, with no detectable organomegaly or palpable masses. Notably, bowel sounds were auscultated within the left hemithorax. On respiratory examination, percussion revealed a dull note over the lower two-thirds of the left hemithorax. Auscultation demonstrated markedly decreased air entry on the left side, confirming the presence of intrathoracic bowel sounds over the left lower thoracic region.
Routine hematological and biochemical investigations were within normal limits. A chest radiograph in the posteroanterior (PA) view revealed a rightward shift of the mediastinum and cardiac silhouette, obscuration of the left costophrenic angle, and multiple air-fluid levels occupying the lower two-thirds of the left hemithorax (Figure 1A). Based on these radiographic findings, a provisional diagnosis of left-sided empyema with associated mediastinal shift was initially considered, and a contrast-enhanced computed tomography (CECT) scan of the thorax was recommended for further evaluation.
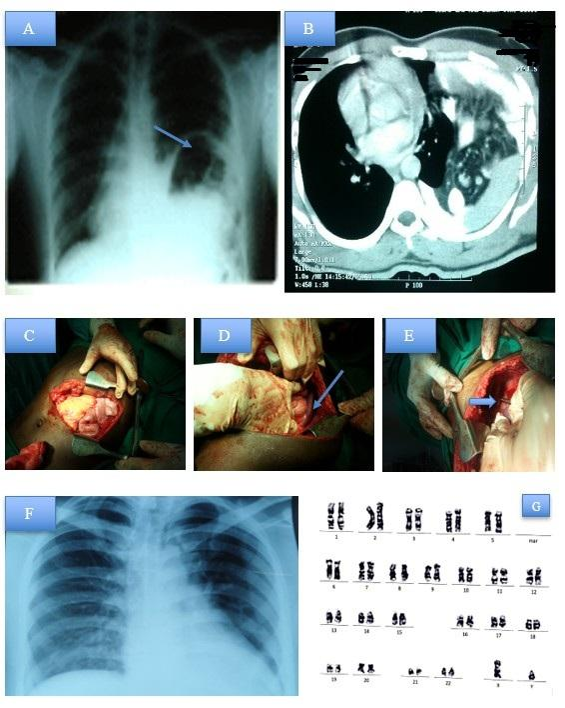
Radiological and intraoperative findings in Case 1 (Bochdalek hernia). (A) Preoperative chest radiograph (PA view) demonstrating a mediastinal shift to the right, obscuration of the left costophrenic angle, and multiple air-fluid levels within the left hemithorax, indicative of herniated bowel. (B) Contrast-enhanced computed tomography (CECT) of the thorax confirming the herniation of abdominal viscera, including the spleen and small intestine, into the left thoracic cavity. (C) Intraoperative view of the left thoraco-abdominal incision utilized for surgical access. (D) Visualization of the spleen located at an abnormally high position within the thoracic apex, with ectopic vascularization (arrow). (E) Intraoperative identification of a hypoplastic left lung (arrow) secondary to chronic compression by herniated viscera. (F) Follow-up chest radiograph at 8 months post-surgery demonstrating complete re-expansion of the left lung and restoration of normal thoracic anatomy. (G) Conventional G-banded karyotype analysis revealing a normal male complement (46,XY), consistent with ISCN guidelines.
Contrast-enhanced computed tomography (CECT) of the thorax provided definitive diagnostic clarification (Figure 1B). The CT scan revealed extensive herniation of abdominal contents into the left thoracic cavity, including the spleen, the splenic flexure of the colon, and loops of the small intestine. A significant mediastinal shift to the right was observed, compressing the adjacent lung parenchyma and displacing the heart. These findings were highly characteristic of a congenital diaphragmatic hernia (CDH), specifically a Bochdalek hernia, presenting unusually in adulthood.
After thorough preoperative evaluation and optimization, the patient was scheduled for surgery, with an initial plan for diagnostic laparoscopy under general anesthesia. On laparoscopic exploration, multiple abdominal viscera were observed herniating through a large defect at the left diaphragmatic hiatus, consistent with a diaphragmatic hernia. However, intraoperative visualization was significantly compromised by dense adhesions at the herniation site, attributable to the chronicity of the condition.
In light of the poor visualization, increased risk of organ injury, and the complexity of the required adhesiolysis, the surgical team decided to convert to an open approach. A thoraco-laparotomy was performed via a left-sided thoraco-abdominal incision at the eighth intercostal space (Figure 1C).
Upon exploration, an unexpected anatomical variant was noted: the spleen was found displaced abnormally high into the thoracic cavity, extending near the apex of the left hemithorax (Figure 1D). Remarkably, the spleen had developed an ectopic collateral vascular supply, deriving its blood flow primarily from hypertrophied intercostal vessels rather than the native splenic artery arising from the celiac trunk. This aberrant vascularization rendered splenic preservation unfeasible due to the high risk of hemorrhage and compromised organ viability. Hence, a splenectomy was performed in a controlled manner. Further inspection revealed a hypoplastic left lung, secondary to long-standing compression by the herniated abdominal contents during development (Figure 1E). The herniated abdominal contents, including the splenic flexure of the colon and small bowel loops, were carefully reduced back into the abdominal cavity.
The diaphragmatic defect was found to be large and was repaired using a dual-sided composite polypropylene mesh. The mesh was anchored securely from the thoracic side using multiple polypropylene (Prolene) stay sutures, ensuring adequate reinforcement of the diaphragmatic musculature and minimizing the risk of recurrence.
A chest tube (intercostal chest drain, ICD) was placed in the eighth intercostal space to facilitate lung re-expansion and evacuate any residual pleural effusion. The procedure concluded uneventfully, and the patient was extubated successfully in the operating room.
The postoperative period was uneventful. The patient was monitored in the surgical intensive care unit (ICU) for 48 hours before being transferred to the surgical ward. The patient remained hemodynamically stable with gradually improving respiratory function. Broad-spectrum antibiotics and postoperative chest physiotherapy were instituted.
The ICD was removed on the twelfth postoperative day following satisfactory lung re-expansion and cessation of pleural drainage. The patient was discharged in stable condition on the 18th postoperative day, with instructions to maintain regular follow-up and receive prophylactic vaccinations against encapsulated organisms (including pneumococcal, Haemophilus influenzae type b, and meningococcal vaccines) secondary to the splenectomy, in accordance with guidelines. The patient was followed up every 3 months for the subsequent 2 to 3 years in the surgical and medical outpatient departments (OPD); no recurrence was observed, and pulmonary function improved significantly.
Given the unusual anatomical findings and the potential possibility of underlying syndromic or chromosomal abnormalities, a conventional karyotyping study was performed, which reported a normal male karyotype (46,XY) after evaluating 20 metaphases (Figure 1G), thereby ruling out any major numerical or structural chromosomal anomaly. The procedural protocols adhered to established international guidelines. Conventional G-banded karyotyping was performed on peripheral blood lymphocytes, analyzing 20 metaphases according to standard International System for Human Cytogenomic Nomenclature (ISCN) guidelines.
Case 2
A 75-year-old female presented with a ten-year history of dyspnea on exertion, a sensation of a "respiratory catch" in the recumbent position, and intermittent palpitations. Over the preceding decade, she had been evaluated by multiple cardiologists and had undergone percutaneous coronary intervention with stenting on two occasions under the presumption that her symptoms were of cardiac etiology; however, her symptoms persisted despite these interventions. The patient denied any history of trauma, chronic respiratory illness, or gastrointestinal disturbances. Furthermore, there was no family history suggestive of congenital anomalies or inheritable disorders.
On clinical examination, she appeared hemodynamically stable. Thoracic examination revealed decreased air entry over the lower half of the right hemithorax. Cardiovascular and abdominal examinations were unremarkable, with normal heart sounds and no audible murmurs.
Routine hematological and biochemical investigations, including a complete blood count, liver and renal function tests, and blood glucose levels, were within normal limits. A retrospective review of her previous chest radiographs, which were initially interpreted as unremarkable, revealed subtle abnormalities that had been overlooked (Figure 2A).
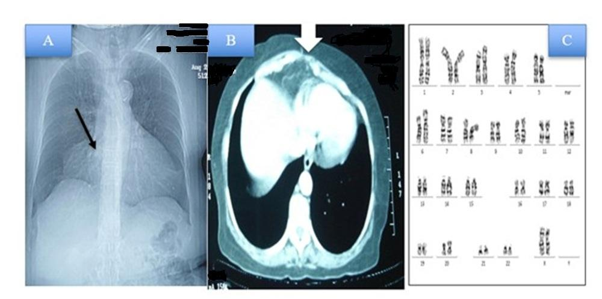
Radiological and cytogenetic evaluation in Case 2 (Morgagni hernia). (A) Preoperative computed tomography (CT) scout film showing subtle right paracardiac abnormalities that were initially overlooked. (B) Axial contrast-enhanced computed tomography (CECT) of the thorax demonstrating a well-defined right paracardiac diaphragmatic defect with isolated herniation of omental fat into the thoracic cavity adjacent to the heart. (C) Conventional G-banded karyotype analysis confirming a normal female chromosomal complement (46,XX) across 20 evaluated metaphases, in accordance with ISCN guidelines.
Contrast-enhanced computed tomography (CECT) of the thorax revealed a well-defined diaphragmatic defect in the right paracardiac region (Figure 2B). Omental fat was observed herniating through the foramen of Morgagni into the right thoracic cavity adjacent to the heart, without associated bowel involvement. Based on these radiological findings, a diagnosis of a right paracardiac Morgagni hernia was established.
Following a thorough preoperative evaluation, the patient underwent an elective laparoscopic repair under general anesthesia. Upon laparoscopic entry into the peritoneal cavity, the omental tissue was identified herniating through the anterior diaphragmatic defect. The herniated contents were carefully reduced into the abdominal cavity. The defect was repaired using a rectangular, Parietex dual-layer composite mesh measuring 9 cm × 10 cm. The mesh comprised a textured, three-dimensional polyester fabric layer on one side and a smooth, absorbable collagen film on the contralateral side. The polyester fabric face was placed against the diaphragm, while the smooth collagen face was oriented toward the abdominal cavity and secured using non-absorbable titanium tacks. The surgical procedure was completed uneventfully, with minimal blood loss and no intraoperative complications.
The patient’s respiratory symptoms improved significantly during the immediate postoperative period. She tolerated early oral intake, mobilized satisfactorily, demonstrated no evidence of recurrence or complications, and was discharged on the tenth postoperative day. The patient was followed up every 3 months for the subsequent 2 to 3 years in the surgical and medical outpatient departments (OPD); no recurrence was observed, and pulmonary function improved significantly.
Given the congenital nature of a Morgagni hernia, the patient underwent a chromosomal evaluation. Conventional karyotyping was performed on peripheral blood lymphocytes, revealing a normal female karyotype of 46,XX across all 20 metaphases (Figure 2C), thereby ruling out any gross chromosomal aberrations. Written informed consent for the publication of clinical details and images was obtained from the patient, ensuring strict anonymity. A structured summary of both case details is provided in Table 1.
Clinical characteristics, anatomical features, surgical management, and cytogenetic profiles of the two presented adult-onset congenital diaphragmatic hernia cases
| S.No | Age | Side | Defect Type | Herniated Contents | Surgical Approach | Outcome |
|---|---|---|---|---|---|---|
| 1. | 26 years (male) | Left | Congenital diaphragmatic hernia (Bochdalek type) | Spleen (ectopically high in thorax with aberrant intercostal vascular supply), splenic flexure of colon, loops of small intestine | Initial diagnostic laparoscopy → converted to open thoraco-laparotomy with diaphragmatic repair using composite mesh; splenectomy performed | Uneventful recovery, hemodynamically stable, improved respiratory function, discharged with chest physiotherapy and antibiotics. vaccination post-splenectomy. Normal Karyotype 46, XY. |
| 2. | 75 years (female) | Right (para cardiac) | Congenital diaphragmatic hernia (Morgagni type) | Omental fat (no bowel involvement) | Elective laparoscopic reduction with composite mesh repair secured with tackers | Uneventful recovery, significant improvement in respiratory symptoms, discharged, no recurrence during 2–3 years of follow-up. Normal karyotype 46, XX. |
Discussion
Bochdalek hernia, which arises from a posterolateral diaphragmatic defect, accounts for over 80% to 85% of CDH cases and is predominantly left-sided, a phenomenon attributed to the earlier closure of the right pleuroperitoneal canal and the protective barrier provided by the liver. Adults with Bochdalek hernias frequently present with nonspecific gastrointestinal or respiratory symptoms, as demonstrated in our first case. Clinical manifestations such as postprandial pain, vomiting, and dyspnea are frequently misinterpreted as gastrointestinal or cardiopulmonary pathologies, thereby delaying definitive diagnosis.
Recent literature highlights the highly heterogeneous clinical presentations of adult Bochdalek hernias. For instance, Gu et al. 7 described a rare adult case presenting with chest pain co-occurring with an intestinal malrotation anomaly, managed successfully via prosthetic patch repair. Similarly, Azhar et al. 8 reported a case characterized by abdominal pain and a choking sensation that was initially misdiagnosed as peptic ulcer disease, but later found to harbor a gastric volvulus within a Bochdalek hernia. These cases underscore the importance of incorporating diaphragmatic hernias into the differential diagnoses for atypical gastrointestinal or respiratory symptoms.
Akita et al. 9 reported two adult Bochdalek hernia cases, highlighting the heightened risk of perioperative cardiopulmonary complications stemming from delayed diagnosis. They emphasized the critical necessity of a thorough preoperative assessment, vigilant intraoperative monitoring, and a multidisciplinary management strategy in adult CDH to prevent severe cardiorespiratory compromise.
Case 1 in our study highlights several unique findings: a massive left-sided Bochdalek hernia with herniation of the spleen, small bowel, and colon, accompanied by ipsilateral pulmonary hypoplasia resulting from long-standing compression. The ectopic splenic vascularization arising from the intercostal arteries is rarely reported and reflects profound chronicity and adaptive vascular remodeling. The need for splenectomy due to non-viability and aberrant blood supply underscores the importance of early diagnosis. This ectopic splenic vascularization observed in our case likely represents adaptive collateral neovascularization secondary to chronic intrathoracic displacement of the spleen. Long-standing herniation and altered anatomical positioning may promote the recruitment and hypertrophy of adjacent intercostal vessels to maintain splenic perfusion, reflecting progressive vascular remodeling over many years. Similar adaptive collateralization in chronically displaced thoracoabdominal viscera has been described in cases of long-standing congenital diaphragmatic defects and intrathoracic spleen 10,11.
Surgical management remains the cornerstone of treatment, with mesh repair often required for large defects. Although minimally invasive approaches are preferred, conversion to an open thoraco-laparotomy, as occurred in this case, may be warranted due to dense adhesions or complex anatomical challenges.
Morgagni hernias, by contrast, occur due to defects in the retrosternal region (foramen of Morgagni) and account for approximately 2% to 4% of CDH cases. They occur more frequently on the right side and commonly contain omental fat, the transverse colon, or the liver. Most Morgagni hernias in adults are incidentally diagnosed during the evaluation of vague symptoms, and their clinical presentation can be highly deceptive.
In Case 2, the patient underwent repeated cardiac interventions, including two coronary stenting procedures, due to the erroneous misattribution of her dyspnea and palpitations to ischemic heart disease. The true etiology—a right-sided Morgagni hernia—was only recognized after persistent symptoms prompted advanced imaging. This emphasizes the necessity of considering diaphragmatic hernias in the differential diagnosis of unexplained cardiopulmonary symptoms, especially in elderly patients with non-resolving symptoms despite standard therapeutic interventions.
Recent studies support the efficacy of minimally invasive surgical approaches for Morgagni hernias. Wadia et al. 12 reported a successful laparoscopic repair of a symptomatic right congenital Morgagni hernia in a 70-year-old female, highlighting the benefits of minimally invasive techniques in elderly patients. Similarly, a 2025 case report detailed a 63-year-old female undergoing laparoscopic repair with mesh reinforcement, resulting in complete symptom resolution and no recurrence at a six-month follow-up 13.
Another critical aspect is the association of CDH with chromosomal and genetic abnormalities. Studies indicate that 18% to 25% of CDH cases are associated with syndromes or chromosomal anomalies, such as trisomy 18, 13, or 21, deletions in 15q26, or microdeletions in 8p23.1 involving the GATA4 gene—a key molecular regulator of diaphragmatic development. Therefore, cytogenetic evaluation through karyotyping remains essential, even in adult cases with late-onset symptoms, to identify syndromic associations or familial patterns 14,15,16.
Both patients in our study underwent conventional karyotyping and were found to have normal chromosomal complements (46,XY and 46,XX, respectively), ruling out gross cytogenetic abnormalities. Although chromosomal abnormalities are reported in syndromic CDH, isolated adult cases rarely demonstrate detectable abnormalities on conventional karyotyping. Therefore, routine karyotyping in all adult CDH cases may not be warranted. Instead, advanced molecular techniques, such as chromosomal microarray analysis (CMA) or whole-exome sequencing, should be reserved for cases with additional congenital anomalies or strong clinical suspicion.
This study is limited by its retrospective nature and the lack of advanced molecular genetic testing (e.g., CMA), which could detect submicroscopic genomic alterations.
Conclusion
In conclusion, these two cases illustrate the highly polymorphic and deceptive clinical presentations of congenital diaphragmatic hernia (CDH) in adulthood. Whereas the first case involved a complex Bochdalek-type hernia characterized by intrathoracic splenic ectopia and secondary pulmonary hypoplasia, the second case masqueraded as ischemic heart disease for a decade before being correctly diagnosed as a Morgagni hernia. Notably, the patient in Case 2 underwent repeated invasive cardiological interventions, further underscoring the risk of diagnostic error when CDH presents with atypical symptoms.
These cases collectively highlight the formidable diagnostic challenges associated with adult CDH. Consequently, maintaining a high index of clinical suspicion coupled with advanced radiological imaging remains the cornerstone of accurate diagnosis. Genetic evaluation should be individualized; while conventional karyotyping may help exclude gross chromosomal abnormalities, higher-resolution techniques, such as chromosomal microarray analysis (CMA) or comparative genomic hybridization (CGH), should be considered when there is a strong clinical suspicion of an underlying genetic etiology.
Abbreviations
AIIMS: All India Institute of Medical Sciences; CDH: Congenital diaphragmatic hernia; CECT: Contrast-enhanced computed tomography; CGH: Comparative genomic hybridization; CMA: Chromosomal microarray analysis; CT: Computed tomography; ICD: Intercostal chest drain; ICU: Intensive care unit; ISCN: International System for Human Cytogenomic Nomenclature; MRI: Magnetic resonance imaging; OPD: Outpatient department; PA: Posteroanterior
Acknowledgments
None.
Author’s contributions
All authors equally contributed to this work, read and approved the final manuscript.
Funding
None.
Availability of data and materials
Data and materials used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics approval and consent to participate
Not applicable.
Consent for publication
Written informed consent was obtained from the patient’s mother for publication of this Case Report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Declaration of generative AI and AI-assisted technologies in the writing process
The authors declare that they have not used generative AI (a type of artificial intelligence technology that can produce various types of content including text, imagery, audio and synthetic data).
Competing interests
The authors declare that they have no competing interests.